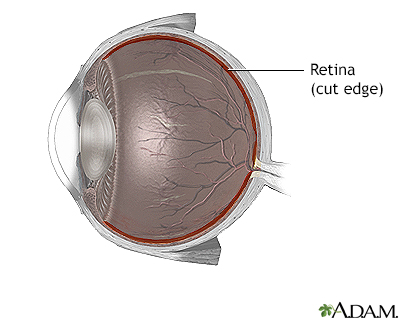
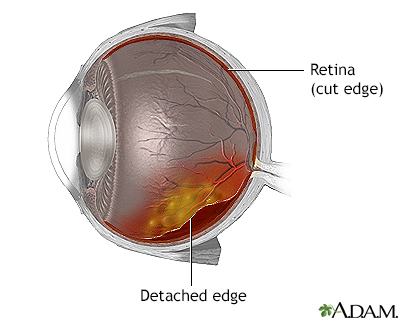
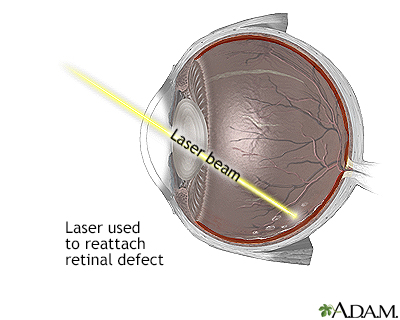
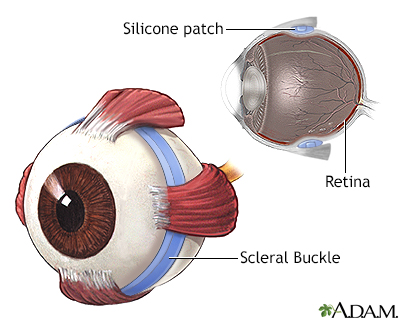
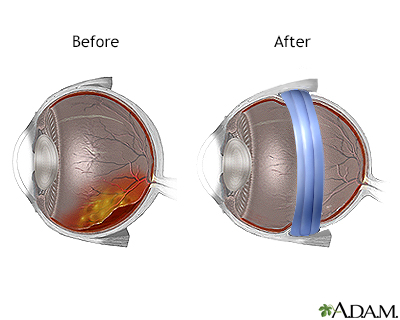
Retinal detachment repair


Review Date:
8/5/2024
Reviewed By: Franklin W. Lusby, MD, Ophthalmologist, Lusby Vision Institute, La Jolla, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
Reviewed By: Franklin W. Lusby, MD, Ophthalmologist, Lusby Vision Institute, La Jolla, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language.
© 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
© 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
All content on this site including text, images, graphics, audio, video, data, metadata, and compilations is protected by copyright and other intellectual property laws. You may view the content for personal, noncommercial use. Any other use requires prior written consent from Ebix. You may not copy, reproduce, distribute, transmit, display, publish, reverse-engineer, adapt, modify, store beyond ordinary browser caching, index, mine, scrape, or create derivative works from this content. You may not use automated tools to access or extract content, including to create embeddings, vectors, datasets, or indexes for retrieval systems. Use of any content for training, fine-tuning, calibrating, testing, evaluating, or improving AI systems of any kind is prohibited without express written consent. This includes large language models, machine learning models, neural networks, generative systems, retrieval-augmented systems, and any software that ingests content to produce outputs. Any unauthorized use of the content including AI-related use is a violation of our rights and may result in legal action, damages, and statutory penalties to the fullest extent permitted by law. Ebix reserves the right to enforce its rights through legal, technological, and contractual measures.
© 1997-
 All rights reserved.
All rights reserved.
All rights reserved.
A.D.A.M. content is best viewed in IE9 or above, Firefox and Google Chrome browser.