Sleep apnea - pediatric; Apnea - pediatric sleep apnea syndrome; Sleep-disordered breathing - pediatric DefinitionWith pediatric sleep apnea, a child's breathing pauses during sleep because the airway has become narrowed or partly blocked. CausesDuring sleep, all of the muscles in the body become more relaxed. This includes the muscles that help keep the throat open so air can flow into the lungs. Normally, the throat remains open enough during sleep to let air pass by. However, some children have a narrow throat. This is often because of large tonsils or adenoids, which partially block the airflow. When the muscles in their upper throat relax during sleep, the tissues close in and block the airway, stopping the breathing. This stop in breathing is called apnea. Other factors that also may increase the risk of sleep apnea in children include:
SymptomsLoud snoring is a telltale symptom of sleep apnea. Snoring is caused by air squeezing through the narrowed or blocked airway. However, not every child who snores has sleep apnea. Children with sleep apnea also have the following symptoms at night:
During the daytime, children with sleep apnea may:
Exams and TestsYour child's health care provider will take your child's medical history and do a physical exam.
Your child may be given a sleep study to confirm sleep apnea. TreatmentSurgery to remove the tonsils and adenoids often cures the condition in children. If needed, surgery also may be used to:
Sometimes, surgery is not recommended or does not help. In that case, your child may use a continuous positive airway pressure (CPAP) device.
It can take some time to get used to sleeping using CPAP therapy. Good follow-up and support from a sleep center can help your child overcome any problems using CPAP. Other treatments may include:
Outlook (Prognosis)In most cases, treatment completely relieves symptoms and problems from sleep apnea. Possible ComplicationsUntreated pediatric sleep apnea may lead to:
When to Contact a Medical ProfessionalContact your provider if:
ReferencesHarsanyi K, Ratarasarn K, Amara AW, Maddox MH. Epidemiology of sleep medicine. In: Kryger M, Roth T, Goldstein CA, Dement WC, eds. Principles and Practice of Sleep Medicine. 7th ed. Philadelphia, PA: Elsevier; 2022:chap 70. Ishman SL, Prosser JD. Evaluation and management of persistent pediatric obstructive sleep apnea. In: Friedman M, Jacobowitz O, eds. Sleep Apnea and Snoring. 2nd ed. Philadelphia, PA: Elsevier; 2020:chap 69. Owens JA, Gueye-Ndiaye S. Sleep medicine. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 31. Sheldon SH. Differential diagnosis in pediatric sleep medicine. In: Sheldon SH, Kryger M, Gozal D, Canapari C, Oyegbile-Chidi TO, eds. Principles and Practice of Pediatric Sleep Medicine. 3rd ed. Elsevier; 2025:chap 8. | ||
| ||
Review Date: 7/1/2025 Reviewed By: Neil K. Kaneshiro, MD, MHA, Clinical Professor of Pediatrics, University of Washington School of Medicine, Seattle, WA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. All content on this site including text, images, graphics, audio, video, data, metadata, and compilations is protected by copyright and other intellectual property laws. You may view the content for personal, noncommercial use. Any other use requires prior written consent from Ebix. You may not copy, reproduce, distribute, transmit, display, publish, reverse-engineer, adapt, modify, store beyond ordinary browser caching, index, mine, scrape, or create derivative works from this content. You may not use automated tools to access or extract content, including to create embeddings, vectors, datasets, or indexes for retrieval systems. Use of any content for training, fine-tuning, calibrating, testing, evaluating, or improving AI systems of any kind is prohibited without express written consent. This includes large language models, machine learning models, neural networks, generative systems, retrieval-augmented systems, and any software that ingests content to produce outputs. Any unauthorized use of the content including AI-related use is a violation of our rights and may result in legal action, damages, and statutory penalties to the fullest extent permitted by law. Ebix reserves the right to enforce its rights through legal, technological, and contractual measures. | ||
| ||


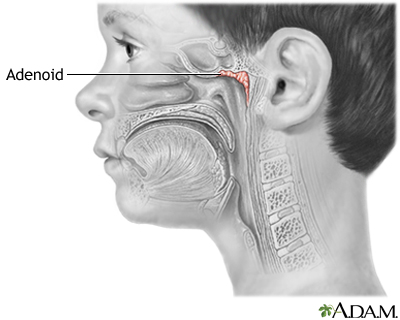 Adenoids
Adenoids