Hysteroscopy - endometrial ablation; Laser thermal ablation; Endometrial ablation - radiofrequency; Endometrial ablation - thermal balloon ablation; Rollerball ablation; Hydrothermal ablation; Novasure ablation DefinitionEndometrial ablation is a surgery or procedure done to disrupt the lining of the uterus in order to minimize heavy or prolonged menstrual flow. This lining is called the endometrium. The surgery may be done in a hospital, outpatient surgery center, or the health care provider's office. DescriptionEndometrial ablation is a procedure used to treat abnormal bleeding by destroying tissue in the uterine lining. The tissue can be removed using:
Some types of procedures are done using a thin, lighted tube called a hysteroscope that sends images of the inside of the womb to a video monitor. Most of the time general anesthesia is used so you will be asleep and pain free. However, newer techniques can be done without using a hysteroscope. For these, a shot of numbing medicine is injected into the nerves around the cervix to block pain. Why the Procedure Is PerformedThis procedure can treat heavy or irregular periods. Your provider will likely have tried other treatments first, such as hormone medicines or an IUD. Endometrial ablation will not be used if you may want to become pregnant in the future. Though this procedure does not prevent you from getting pregnant, it may reduce your chances of getting pregnant. Reliable contraception is important in all women who get the procedure. If a woman gets pregnant after an ablation procedure, the pregnancy will often miscarry or be extremely high risk because of the scar tissue in the uterus. RisksRisks of hysteroscopy include:
Risks of ablation procedures vary depending on the method used. Risks may include:
Risks of any pelvic procedure include:
Risks of anesthesia include:
Risks of any procedure include:
Before the ProcedureA biopsy of the endometrium or lining of the uterus will be performed in the weeks prior to the procedure. Younger women may be treated with a hormone that blocks estrogen from being made by the body for 1 to 3 months before the procedure. Your provider may prescribe medicine to open your cervix. This makes it easier to insert the scope. You need to take this medicine about 8 to 12 hours before your procedure. Before the procedure, tell your provider:
During the week before your surgery:
On the day of the procedure:
After the ProcedureYou may go home the same day. Rarely, you may need to stay overnight.
Your provider will tell you the results of your procedure. Outlook (Prognosis)The lining of your uterus heals by scarring. Women will most often have less menstrual bleeding after this procedure. Up to 30% to 50% of women will completely stop having periods. This result is more likely in older women. Women who continue to have heavy bleeding may need additional surgery. ReferencesBaggish MS. Minimally invasive nonhysteroscopic endometrial ablation. In: Baggish MS, Karram MM, eds. Atlas of Pelvic Anatomy and Gynecologic Surgery. 5th ed. Philadelphia, PA: Elsevier; 2021:chap 107. Kintanar TA. Endometrial ablation. In: Fowler GC, ed. Pfenninger and Fowler's Procedures for Primary Care. 4th ed. Philadelphia, PA: Elsevier; 2020:chap 133. Raymond L, Lentz GM. Endoscopy in minimally invasive gynecologic surgery. In: Gershenson DM, Lentz GM, Valea FA, Lobo RA, eds. Comprehensive Gynecology. 8th ed. Philadelphia, PA: Elsevier; 2022:chap 10. | ||
| ||
Review Date: 10/15/2024 Reviewed By: John D. Jacobson, MD, Professor Emeritus, Department of Obstetrics and Gynecology, Loma Linda University School of Medicine, Loma Linda, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


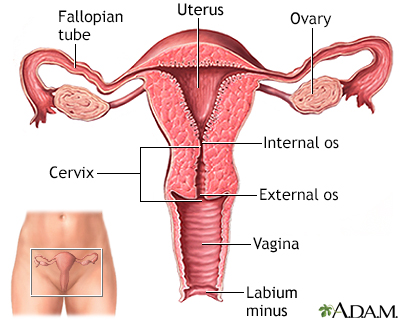 Uterus
Uterus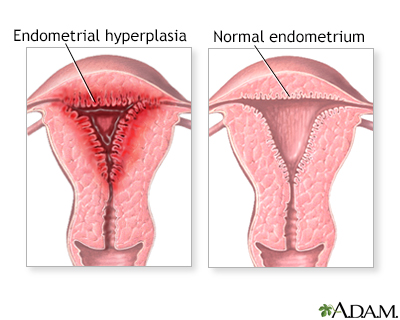 Abnormal menstrual...
Abnormal menstrual...