Globus pallidus deep brain stimulation; Subthalamic deep brain stimulation; Thalamic deep brain stimulation; DBS; Brain neurostimulation DefinitionDeep brain stimulation (DBS) uses a device called a neurostimulator to deliver electrical signals to the areas of the brain that control movement, pain, mood, weight, obsessive-compulsive thoughts, and awakening from a coma. DescriptionThe DBS system consist of four parts:
Surgery is done to place each part of the neurostimulator system. In adults, the whole system can be placed in 1 or 2 stages (two separate surgeries). Stage 1 is usually done under local anesthesia, meaning you are awake, but pain-free. (In children, general anesthesia is given.)
Stage 2 is done under general anesthesia, meaning you are asleep and pain-free. The timing of this stage of surgery depends on where in the brain the stimulator will be placed.
Once connected, electric pulses travel from the neurostimulator, along the extension wire, to the lead, and into the brain. These tiny pulses interfere with and block the electrical signals that cause symptoms of certain diseases. Why the Procedure Is PerformedDBS is commonly done for people with Parkinson disease when the symptoms cannot be controlled by medicines. DBS does not cure Parkinson disease, but can help reduce symptoms such as:
DBS may also be used to treat the following conditions:
RisksDBS is considered safe and effective when done in the right people. Risks of DBS placement may include:
Problems may also occur if parts of the DBS system break or move. These include:
Possible risks of any brain surgery are:
Risks of general anesthesia are:
Before the ProcedureYou will have a complete physical exam. Your surgeon will order many laboratory and imaging tests, including a CT or MRI scan. These imaging tests are done to help the surgeon pinpoint the exact part of the brain responsible for the symptoms. The images are used to help the surgeon place the lead in the brain during surgery. You might have to see more than one specialist, such as a neurologist, neurosurgeon, or psychologist, to make sure that the procedure is right for you and has the best chance of success. Before surgery, tell your surgeon:
Planning for your surgery:
During the week before the surgery:
The night before and on the day of surgery, follow instructions about:
After the ProcedureYou may need to stay in the hospital for about 3 days. Your surgeon may prescribe antibiotics to prevent infection. You will return to your surgeon's office at a later date after surgery. During this visit, the stimulator is turned on and the amount of stimulation is adjusted. Surgery is not needed. This process is also called programming. Contact your surgeon if you develop any of the following after DBS surgery:
Outlook (Prognosis)People who have DBS usually do well during the surgery. Many people have great improvement in their symptoms and quality of life. Most people still need to take medicine, but at a lower dosage. This surgery, and surgery in general, is riskier in people over age 70 and those with health conditions such as high blood pressure and diseases that affect blood vessels in the brain. You and your health care provider should carefully weigh the benefits of this surgery against the risks. The DBS procedure can be reversed, if needed. ReferencesGehl C, Paulsen JS. Behavior and personality disturbances. In: Newman NJ, Jankovic J, Mazziotta JC, Pomeroy SL, eds. Bradley and Daroff's Neurology in Clinical Practice. 8th ed. Philadelphia, PA: Elsevier; 2022:chap 9. Johnson LA, Vitek JL. Deep brain stimulation: mechanisms of action. In: Winn HR, ed. Youmans and Winn Neurological Surgery. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 113. Krauss JK, Lipsman N, Aziz T. et al. Technology of deep brain stimulation: current status and future directions. Nat Rev Neuro. 2021;17:75-87. www.ncbi.nlm.nih.gov/pmc/articles/PMC7116699/. Lozano AM, Lipsman N, Bergman H, et al. Deep brain stimulation: current challenges and future directions. Nat Rev Neurol. 2019;15(3):148-160. PMID: 30683913 pubmed.ncbi.nlm.nih.gov/30683913/. | ||
| ||
Review Date: 12/31/2023 Reviewed By: Luc Jasmin, MD, Ph.D., FRCS (C), FACS, Department of Neuroscience, Guam Regional Medical City, Guam; Department of Surgery, Johnson City Medical Center, TN; Department of Maxillofacial Surgery at UCSF, San Francisco, CA. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. Editorial update 05/28/2025. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


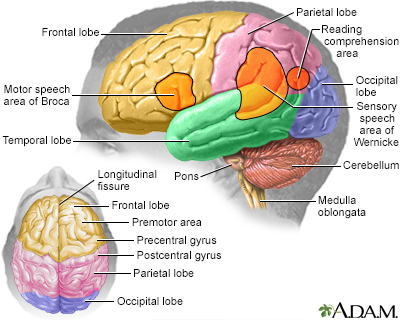 Brain
Brain