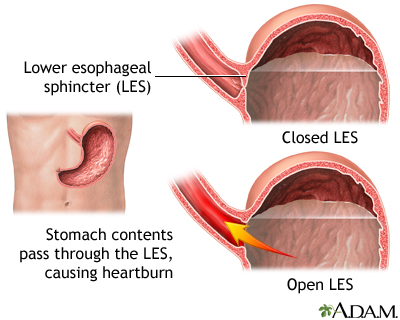
Fundoplication - children; Nissen fundoplication - children; Belsey (Mark IV) fundoplication - children; Toupet fundoplication - children; Thal fundoplication - children; Hiatal hernia repair - children; Endoluminal fundoplication - children DefinitionAnti-reflux surgery is surgery to tighten the muscles at the bottom of the esophagus (the tube that carries food from the mouth to the stomach). Problems with these muscles can lead to gastroesophageal reflux disease (GERD). This surgery can also be done during a hiatal hernia repair. This article discusses anti-reflux surgery in children. DescriptionThe most common type of anti-reflux surgery is called fundoplication. This surgery most often takes 2 to 3 hours. Your child will be given general anesthesia before the surgery. That means the child will be asleep and unable to feel pain during the procedure. The surgeon will use stitches to wrap the upper part of your child's stomach around the end of the esophagus. This helps prevent stomach acid and food from flowing back up. A gastrostomy tube (g-tube) may be put in place if your child has had swallowing or feeding problems. This tube helps with feeding and releases air from your child's stomach. Another surgery, called pyloroplasty may also be done. This surgery widens the opening between the stomach and small intestine so the stomach can empty faster. This surgery may be done several ways, including:
The surgeon may need to switch to an open procedure if there is bleeding, a lot of scar tissue from earlier surgeries, or if the child is very overweight. Endoluminal fundoplication is similar to a laparoscopic repair, but the surgeon reaches the stomach by going through the mouth. Small clips are used to tighten the connection between the stomach and esophagus. Why the Procedure Is PerformedAnti-reflux surgery is usually done to treat GERD in children only after medicines have not worked or complications develop. Your child's health care provider may suggest anti-reflux surgery when:
RisksRisks for any surgery include:
Risks for anesthesia include:
Anti-reflux surgery risks include:
Before the ProcedureAlways make sure your child's health care provider know what medicines your child is taking including medicines, drugs, herbs, and vitamins you bought without a prescription. Planning for your child's surgery:
During the week before surgery:
On the day of the surgery:
After the ProcedureHow long your child stays in the hospital depends on how the surgery was done.
Your child can start eating again about 1 to 2 days after surgery. Liquids are usually given first. Some children have a g-tube placed during surgery. This tube can be used for liquid feedings, or to release gas from the stomach. If your child did not have a g-tube placed, a tube may be inserted through the nose to the stomach to help release gas. This tube is removed once your child starts eating again. Your child will be able to go home once they are eating food, have had a bowel movement and are feeling better. Outlook (Prognosis)Heartburn and related symptoms should improve after anti-reflux surgery. However, your child may still need to take medicines for heartburn after surgery. Some children may need another operation in the future to treat new reflux symptoms or swallowing problems. This may happen if the stomach was wrapped around the esophagus too tightly or it loosens. The surgery may not be successful if the repair was too loose. ReferencesChun RH, Noel RJ, Arvedson JC. Pediatric swallowing, laryngopharyngeal and gastroesophageal reflux disease, eosinophilic esophagitis, and aspiration. In: Flint PW, Francis HW, Haughey BH, et al, eds. Cummings Otolaryngology: Head and Neck Surgery. 7th ed. Philadelphia, PA: Elsevier; 2021:chap 212. Holcomb GW. Gastroesophageal reflux. In: Holcomb GW, Murphy JP, St. Peter SD, eds. Holcomb and Ashcraft's Pediatric Surgery. 7th ed. Philadelphia, PA: Elsevier; 2020:chap 28. Khan S, Matta SKR. Gastroesophageal reflux disease. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 369. | ||
| ||
Review Date: 1/17/2025 Reviewed By: Charles I. Schwartz, MD, FAAP, Clinical Assistant Professor of Pediatrics, Perelman School of Medicine at the University of Pennsylvania, General Pediatrician at PennCare for Kids, Phoenixville, PA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


 Gastroesophageal r...
Gastroesophageal r...