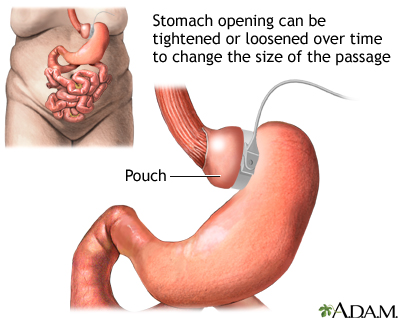
Lap-Band; LAGB; Laparoscopic adjustable gastric banding; Bariatric surgery - laparoscopic gastric banding; Obesity - gastric banding; Weight loss - gastric banding DefinitionLaparoscopic gastric banding is surgery to help with weight loss. The surgeon places a band around the upper part of your stomach to create a small pouch to hold food. The band limits the amount of food you can eat by making you feel full after eating small amounts of food. After surgery, your surgeon can adjust the band to make food pass more slowly or quickly through your stomach. Gastric bypass surgery is a related topic. DescriptionYou will receive general anesthesia before this surgery. You will be asleep and unable to feel pain. The surgery is done using a tiny camera that is placed in your belly. This type of surgery is called laparoscopy. The camera is called a laparoscope. It allows your surgeon to see inside your belly. In this surgery:
When you eat after having this surgery, the small pouch will fill up quickly. You will feel full after eating just a small amount of food. The food in the small upper pouch will slowly empty into the main part of your stomach. Why the Procedure Is PerformedWeight-loss surgery (also called metabolic and bariatric surgery or MBS) may be an option if you have moderate to high-risk obesity and have not been able to lose enough weight through diet and exercise. Health care providers often use the body mass index (BMI) and health conditions such as type 2 diabetes (diabetes that started in adulthood) and high blood pressure to determine which people are most likely to benefit from MBS. Laparoscopic gastric banding is not a "quick fix" for obesity. It will greatly change your lifestyle. You must diet and exercise after this surgery. If you do not, you may have complications or poor weight loss. People who have this surgery should be mentally stable and not be dependent on alcohol or illegal drugs. Be sure to discuss the benefits and risks with your surgeon. This procedure may be recommended for the following people with obesity. People with a BMI of 35 or more. Someone with a BMI of 35 or more is 80 or more pounds (36.3 kilograms) over their recommended weight. A healthy BMI is 18.5 to 24.9. People who are Asian who have a BMI of 27.5 or more. Health risks in Asian people occur at a lower BMI than in non-Asian people. People with a BMI of 30 to 34.9 (or a BMI of 25 or more in people who are Asian) who also have a serious medical condition that might improve with weight loss. Some of these conditions are:
RisksRisks for anesthesia and any surgery include:
Risks for gastric banding are:
Before the ProcedureYour surgeon will ask you to have tests and visits with your other providers before you have this surgery. Some of these are:
If you are a smoker, you should stop smoking several weeks before surgery and not start smoking again after surgery. Smoking slows recovery and increases the risk for problems after surgery. Tell your provider if you need help quitting. Always tell your provider:
During the week before your surgery:
On the day of your surgery:
Your provider will tell you when to arrive at the hospital. After the ProcedureYou will probably go home the day of surgery. Many people are able to begin their normal activities 1 or 2 days after going home. Most people take 1 week off from work. You will stay on liquids or mashed-up foods for 2 or 3 weeks after surgery. You will slowly add soft foods, then regular foods, to your diet. By 6 weeks after surgery, you will probably be able to eat regular foods. The band is made of a special rubber (silastic rubber). The inside of the band has an inflatable balloon. This allows the band to be adjusted. You and your surgeon can decide to loosen or tighten it in the future so you can eat more or less food. The band is connected to an access port that is under the skin on your belly. The band can be tightened by placing a needle into the port and filling the balloon (band) with water. Your surgeon can make the band tighter or looser any time after you have this surgery. It may be tightened or loosened if you are:
Outlook (Prognosis)The final weight loss with gastric banding is not as large as with other weight loss surgery. The average weight loss is about one-third to one-half of the extra weight you are carrying. This may be enough for many people. Talk with your provider about which procedure is best for you. In most cases, the weight will come off more slowly than with other weight loss surgery. You may keep losing weight for up to 3 years. Losing enough weight after surgery can improve many medical conditions you might also have, such as:
Weighing less should also make it much easier for you to move around and do your everyday activities. This surgery alone is not a solution to losing weight. It can train you to eat less, but you still have to do much of the work. To lose weight and avoid complications from the procedure, you will need to follow the exercise and eating guidelines that your provider and dietitian gave you. ReferencesMechanick JI, Apovian C, Brethauer S, et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient 2019 update: cosponsored by American Association of Clinical Endocrinologists/American College of Endocrinology, the Obesity Society, American Society for Metabolic & Bariatric Surgery, Obesity Medicine Association, and American Society of Anesthesiologists. Surg Obes Relat Dis. 2020;16(2):175-247. PMID: 31917200 pubmed.ncbi.nlm.nih.gov/31917200/. Powell-Wiley TM, Poirier P; American Heart Association Council on Lifestyle and Cardiometabolic Health, et al. Obesity and cardiovascular disease: A scientific statement from the American Heart Association. Circulation. 2021:143(21):e984-e1010. PMID: 33882682. pubmed.ncbi.nlm.nih.gov/33882682/. Richards WO, Khaitan L, Torquati A. Morbid obesity. In: Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 21st ed. St Louis, MO: Elsevier; 2022:chap 48. Sullivan S, Edmundowicz SA, Morton JM. Surgical and endoscopic treatment of obesity. In: Feldman M, Friedman LS, Brandt LJ, eds. Sleisenger and Fordtran's Gastrointestinal and Liver Disease. 11th ed. Philadelphia, PA: Elsevier; 2021:chap 8. | ||
| ||
Review Date: 7/22/2024 Reviewed By: John E. Meilahn, MD, General and Bariatric Surgery, Wyndmoor, PA. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


 Adjustable gastric...
Adjustable gastric...