Spinal microdiskectomy; Microdecompression; Laminotomy; Disk removal; Spine surgery - diskectomy; Discectomy DefinitionDiskectomy is surgery to remove all or part of the cartilage cushion that helps support part of your spinal column. These cushions are called disks, and they separate your spinal bones (vertebrae). DescriptionYour surgeon may perform disk removal (diskectomy) in these different ways.
Microdiskectomy is done in a hospital or outpatient surgical center. You will be given general anesthesia. You will be asleep and pain-free.
Diskectomy and laminotomy are usually done in a hospital or outpatient surgical center, using general anesthesia (asleep and pain-free).
Why the Procedure Is PerformedWhen one of your disks moves out of place (herniates), the soft gel inside pushes through the wall of the disk. The disk may then place pressure on the spinal cord and nerves that are coming out of your spinal column. Many of the symptoms caused by a herniated disk get better or go away over time without surgery. Most people with low back or neck pain, numbness, or even mild weakness are often first treated with anti-inflammatory medicines, physical therapy, and exercise. Only a few people with a herniated disk need surgery. Your health care provider may recommend a diskectomy if you have a herniated disk and:
If you are having problems with your bowels or bladder, or the pain is so bad that strong pain medicines do not help, you will need to have surgery right away. RisksRisks of anesthesia and surgery in general are:
Risks of this surgery are:
Before the ProcedureTell your surgeon or nurse if:
Planning for your surgery:
During the week before your surgery:
On the day of the surgery:
After the ProcedureYour surgeon will ask you to get up and walk around as soon as your anesthesia wears off. Most people go home the day of surgery. Do not drive yourself home. Follow instructions about how to care for yourself at home. Outlook (Prognosis)Most people have pain relief and can move better after surgery. Numbness and tingling should get better or disappear. Your pain, numbness, or weakness may not get better or go away if you had nerve damage before surgery, or if you have symptoms caused by other spinal conditions. Further changes may occur in your spine over time and new symptoms may occur. Talk with your provider about how to prevent future back problems. ReferencesDixit R. Low back pain. In: Firestein GS, McInnes IB, Koretzky GA, Mikuls TR, Neogi T, O'Dell JR, eds. Firestein & Kelley's Textbook of Rheumatology. 12th ed. Philadelphia, PA: Elsevier; 2025:chap 47. Gardocki RJ. Anatomic approaches to the spine. In: Azar FM, Beaty JH, eds. Campbell's Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021:chap 37. Gardocki RJ, Park AL. Degenerative disorders of the thoracic and lumbar spine. In: Azar FM, Beaty JH, eds. Campbell's Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021:chap 39. Ryu WHA, O’Toole JE. Cervical spine and cervicothoracic junction - anterior approach. In: Steinmetz MP, Berven SH, Benzel EC, eds. Benzel's Spine Surgery. 5th ed. Philadelphia, PA: Elsevier; 2022:chap 109. | ||
| ||
Review Date: 6/4/2025 Reviewed By: C. Benjamin Ma, MD, Professor, Chief, Sports Medicine and Shoulder Service, UCSF Department of Orthopaedic Surgery, San Francisco, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


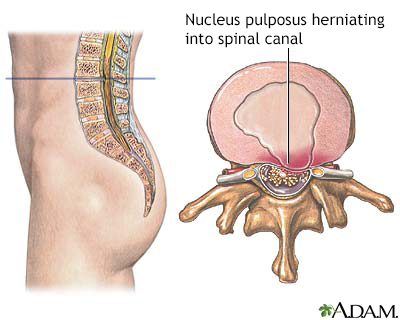 Herniated nucleus ...
Herniated nucleus ...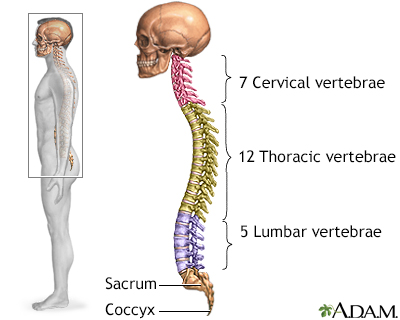 Skeletal spine
Skeletal spine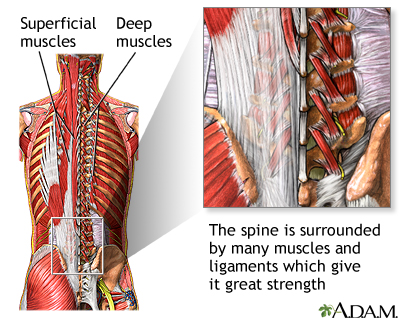 Spine supporting s...
Spine supporting s... Cauda equina
Cauda equina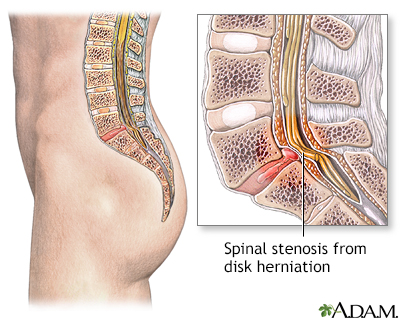 Spinal stenosis
Spinal stenosis