Minimally invasive direct coronary artery bypass; MIDCAB; Robot-assisted coronary artery bypass; RACAB; Keyhole heart surgery; CAD - MIDCAB; Coronary artery disease - MIDCAB DefinitionHeart bypass surgery creates a new route, called a bypass, for blood and oxygen to reach your heart. Minimally invasive coronary (heart) artery bypass can be done without stopping the heart. Therefore, you do not need to be put on a heart-lung machine for this procedure. DescriptionTo perform this surgery:
You will not be on a heart-lung machine for this surgery. However, you will have general anesthesia so you will be asleep and not feel pain. A device will be attached to your heart to stabilize it. You will also receive medicine to slow the heart down. You may have a tube in your chest for drainage of fluid. This will be removed in a day or two. Why the Procedure Is PerformedYour health care provider may recommend a minimally invasive coronary artery bypass if you have a blockage in one or two coronary arteries, most often in the front of the heart. When one or more of the coronary arteries become partly or totally blocked, your heart does not get enough blood. This is called ischemic heart disease or coronary artery disease. It can cause chest pain (angina). Your provider may have first tried to treat you with medicines. You may have also tried cardiac rehabilitation or other treatments, such as angioplasty with stenting. Coronary artery disease varies from person to person. Heart bypass surgery is just one type of treatment. It is not right for everyone. Surgeries or procedures that may be done instead of minimally invasive heart bypass are: RisksYour provider will talk to you about the risks of surgery. In general, the complications of minimally invasive coronary artery bypass are lower than with open coronary artery bypass surgery. Risks related to any surgery include:
Possible risks of coronary artery bypass include:
Before the ProcedureAlways tell your surgeon what medicines you are taking, even drugs or herbs you bought without a prescription. During the days before the surgery:
The day before your surgery:
On the day of the surgery:
Your surgeon will tell you when to arrive at the hospital. After the ProcedureYou may be able to leave the hospital 2 or 3 days after your surgery. The surgeon or nurse will tell you how to care for yourself at home. You may be able to return to normal activities after 2 or 3 weeks. Outlook (Prognosis)Recovery from surgery takes time, and you may not see the full benefits of your surgery for 3 to 6 months. In most people who have heart bypass surgery, the grafts remain open and work well for many years. This surgery does not prevent a blockage from coming back. However, you can take steps to slow it down. Things you can do include:
You may be more likely to have problems with your blood vessels if you have kidney disease or other medical problems. ReferencesOmer S, Bakaeen FG. Acquired heart disease: coronary insufficiency. In: Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 21st ed. Philadelphia, PA: Elsevier; 2022:chap 60. Qureshi SH, Guo MH, Ruel M.. Less -invasive and robotic approaches to coronary artery bypass grafting. In: Sellke FW, del Nido PJ, Swanson SJ, eds. Sabiston and Spencer Surgery of the Chest. 10th ed. Philadelphia, PA: Elsevier; 2024:chap 94.. 2nd ed. Philadelphia, PA: Elsevier; 2019:chap 5. Rodriguez ML, Ruel M. Minimally invasive coronary artery bypass grafting. In: Sellke FW, Ruel M, eds. Atlas of Cardiac Surgical Techniques. 2nd ed. Philadelphia, PA: Elsevier; 2019:chap 5. Writing Committee Members; Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79 (2):e21-e129. PMID: 34895950 pubmed.ncbi.nlm.nih.gov/34895950/. | ||
| ||
Review Date: 5/13/2024 Reviewed By: Mary C. Mancini, MD, PhD, Cardiothoracic Surgeon, Shreveport, LA. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


 Heart - front view
Heart - front view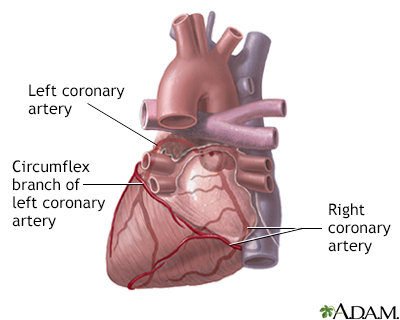 Posterior heart ar...
Posterior heart ar...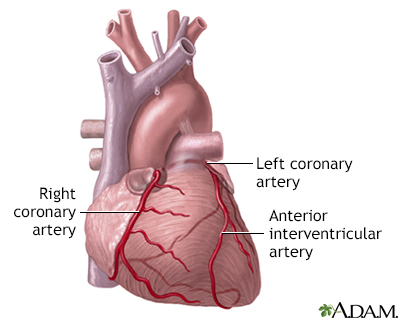 Anterior heart art...
Anterior heart art...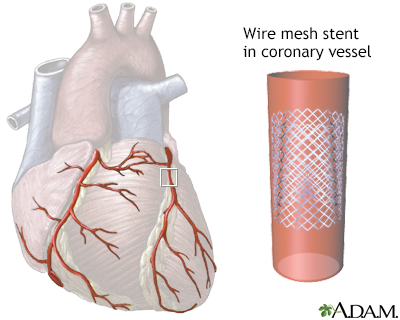 Coronary artery st...
Coronary artery st...