Biopsy - colposcopy - directed; Biopsy - cervix - colposcopy; Endocervical curettage; ECC; Cervical punch biopsy; Biopsy - cervical punch; Cervical biopsy; Cervical intraepithelial neoplasia - colposcopy; CIN - colposcopy; Precancerous changes of the cervix - colposcopy; Cervical cancer - colposcopy; Squamous intraepithelial lesion - colposcopy; LSIL - colposcopy; HSIL - colposcopy; Low-grade colposcopy; High-grade colposcopy; Carcinoma in situ - colposcopy; CIS - colposcopy; ASCUS - colposcopy; Atypical glandular cells - colposcopy; AGUS - colposcopy; Atypical squamous cells - colposcopy; Pap smear - colposcopy; HPV - colposcopy; Human papilloma virus - colposcopy; Cervix - colposcopy; Colposcopy DefinitionA colposcopy is a special way of looking at the cervix. The cervix is the lower part of the uterus (womb) that opens at the top of the vagina. Abnormal changes in the cells on the surface of your cervix is called cervical dysplasia. Colposcopy uses a light and a low-powered microscope to make the cervix appear much larger. This helps your health care provider find and then biopsy abnormal areas in your cervix. How the Test is PerformedYou will lie on a table and place your feet in stirrups, to position your pelvis for exam. The provider will place an instrument (called a speculum) into your vagina to see the cervix clearly. The cervix and vagina are gently cleaned with a vinegar or iodine solution. This removes the mucus that covers the surface and highlights abnormal areas. The provider will place the colposcope at the opening of your vagina and examine the area. Photographs may be taken. The colposcope does not touch you. If any areas look abnormal, a small sample of the tissue will be removed using small biopsy tools. Several samples may be taken. Sometimes a tissue sample from inside the cervix is removed. This is called endocervical curettage (ECC). How to Prepare for the TestThere is no special preparation. You may be more comfortable if you empty your bladder and bowel before the procedure. Before the exam:
This test should not be done during a heavy period, unless it is abnormal. Keep your appointment if you are:
You may be able to take ibuprofen or acetaminophen (Tylenol) before the colposcopy. Ask your provider if this is OK, and when and how much you should take. How the Test will FeelYou may have some discomfort when the speculum is placed inside your vagina. It may be more uncomfortable than a regular Pap test.
Some women may hold their breath during pelvic procedures because they expect pain. Slow, regular breathing will help you relax and relieve pain. Ask your provider about bringing a support person with you if that will help. You may have some bleeding after the biopsy, for about 2 days.
Why the Test is PerformedColposcopy is done to detect cervical cancer and changes that may lead to cervical cancer. It is most often done when you have had an abnormal Pap smear or HPV test. It may also be recommended if you have bleeding after sexual intercourse. Colposcopy may also be done when your provider sees abnormal areas on your cervix during a pelvic exam. These may include:
The colposcopy may be used to keep track of HPV, and to look for abnormal changes that can come back after treatment. Normal ResultsA smooth, pink surface of the cervix is normal. A specialist called a pathologist will examine the tissue sample from the cervical biopsy and send a report to your provider. Biopsy results most often take 1 to 2 weeks. A normal result means there is no cancer and no abnormal changes were seen. What Abnormal Results MeanYour provider should be able to tell you if anything abnormal was seen during the test, including:
Abnormal biopsy results may be due to changes that can lead to cervical cancer. These changes are called dysplasia, or cervical intraepithelial neoplasia (CIN).
Abnormal biopsy results may be due to:
If the biopsy does not determine the cause of abnormal results, you may need a procedure called a cold knife cone biopsy. RisksAfter the biopsy, you may have some bleeding for up to a week. You may have mild cramping, your vagina may feel sore, and you may have a dark discharge for 1 to 3 days. A colposcopy and biopsy will not make it more difficult for you to become pregnant, or cause problems during pregnancy. Contact your provider right away if:
ReferencesBixel K, Ramaswamy B, Christian B, Cohn DE. Malignancy and pregnancy. In: Lockwood CJ, Copel JA, Dugoff L, et al, eds. Creasy and Resnik's Maternal-Fetal Medicine: Principles and Practice. 9th ed. Philadelphia, PA: Elsevier; 2023:chap 56. Khan MJ, Werner CL, Darragh TM, et al. ASCCP colposcopy standards: role of colposcopy, benefits, potential harms and terminology for colposcopic practice. Journal of Lower Genital Tract Disease. 2017;21(4):223-229. PMID: 28953110 pubmed.ncbi.nlm.nih.gov/28953110/. Newkirk GR. Colposcopic examination. In: Fowler GC, ed. Pfenninger and Fowler's Procedures for Primary Care. 4th ed. Philadelphia, PA: Elsevier; 2020:chap 124. Salcedo MP, Phoolcharoen N, Schmeler KM. Intraepithelial neoplasia of the lower genital tract (cervix, vagina, vulva): etiology, screening, diagnosis, management. In: Gershenson DM, Lentz GM, Valea FA, Lobo RA, eds. Comprehensive Gynecology. 8th ed. Philadelphia, PA: Elsevier; 2022:chap 29. | ||
| ||
Review Date: 3/31/2024 Reviewed By: LaQuita Martinez, MD, Department of Obstetrics and Gynecology, Emory Johns Creek Hospital, Alpharetta, GA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


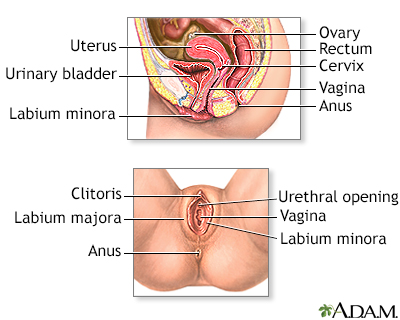 Female reproductiv...
Female reproductiv...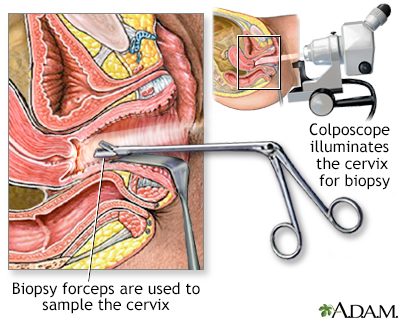 Colposcopy-directe...
Colposcopy-directe...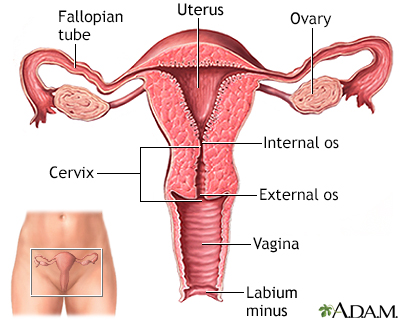 Uterus
Uterus