Leukocyte count; White blood cell count; White blood cell differential; WBC differential; Infection - WBC count; Cancer - WBC count DefinitionA WBC count is a blood test to measure the number of white blood cells (WBCs) in the blood. It is a part of a complete blood count (CBC). WBCs are also called leukocytes. They help fight infections. There are five major types of white blood cells:
How the Test is PerformedA blood sample is needed. How to Prepare for the TestMost of the time, you do not need to take special steps before this test. Tell your health care provider the medicines you are taking, including the ones without a prescription. Some medicines may change the test results. How the Test will FeelWhen the needle is inserted to draw blood, some people feel moderate pain. Others feel only a prick or stinging. Afterward, there may be some throbbing or slight bruising. This soon goes away. Why the Test is PerformedYou will have this test to find out how many WBCs you have. Your provider may order this test to help diagnose conditions such as:
Normal ResultsThe normal number of WBCs in the blood is 4,500 to 11,000 WBCs per microliter (4.5 to 11.0 × 109/L). Normal value ranges may vary slightly among different labs. Some labs use different measurements or may test different specimens. Talk to your provider about your test results. What Abnormal Results MeanLOW WBC COUNT A low number of WBCs is called leukopenia. A count less than 4,500 cells per microliter (4.5 × 109/L) is below normal. Neutrophils are one type of WBC. They are important for fighting infections. A lower than normal WBC count may be due to:
HIGH WBC COUNT A higher than normal WBC count is called leukocytosis. It may be due to:
There may also be less common reasons for abnormal WBC counts. Medicines that may lower your WBC count include:
Medicines that may increase WBC counts include:
RisksThere is little risk involved with having your blood taken. Veins and arteries vary in size from one person to another, and from one side of the body to the other. Obtaining a blood sample from some people may be more difficult than from others. Other risks associated with having blood drawn are slight, but may include:
ReferencesBain BJ. The peripheral blood smear. In: Goldman L, Cooney KA , eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 143. Marcogliese AN, Hensch L. Resources for the hematologist: interpretive comments and selected reference values for neonatal, pediatric, and adult populations. In: Hoffman R, Benz EJ, Silberstein LE, et al, eds. Hematology: Basic Principles and Practice. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 159. Nasr MR, Hutchison RE. Leukocytic disorders. In: McPherson RA, Pincus MR, eds. Henry's Clinical Diagnosis and Management by Laboratory Methods. 24th ed. Philadelphia, PA: Elsevier; 2022:chap 34. Tsai FD, Khanna-Gupta A, Berliner N. Granulocytopoiesis and monocytopoiesis. In: Hoffman R, Benz EJ, Silberstein LE, et al, eds. Hematology: Basic Principles and Practice. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 28. Vajpayee N, Graham SS, Bem S. Basic examination of blood and bone marrow. In: McPherson RA, Pincus MR, eds. Henry's Clinical Diagnosis and Management by Laboratory Methods. 24th ed. Philadelphia, PA: Elsevier; 2022:chap 31. | ||
| ||
Review Date: 2/3/2025 Reviewed By: Warren Brenner, MD, Oncologist, Lynn Cancer Institute, Boca Raton, FL. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


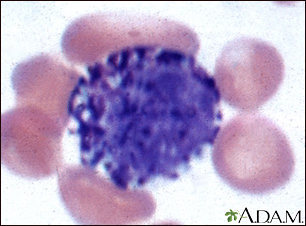 Basophil (close-up
Basophil (close-up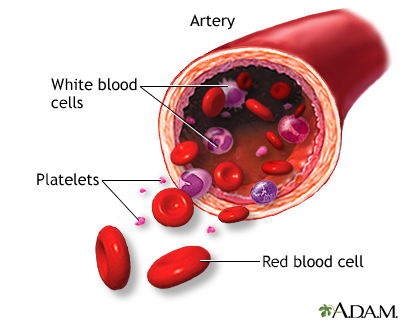 Formed elements of...
Formed elements of...