Baby rash; Miliaria; Prickly heat DefinitionA rash is a change in the color or texture of the skin. A skin rash can be:
ConsiderationsMost bumps and blotches on a newborn baby are harmless and clear up by themselves. The most common skin problem in infants is diaper rash. Diaper rash is an irritation of the skin caused by dampness, urine, or feces. Most babies who wear diapers will have some type of diaper rash at some point. Other skin disorders can cause rashes. These are most often not serious unless they occur with other symptoms. CausesCauses may include:
Home CareDIAPER RASHES Keep the skin dry. Change wet diapers as quickly as possible. Allow the baby's skin to air dry as long as is practical. Launder cloth diapers in mild soap and rinse well. Avoid using plastic pants. Avoid irritating wipes (especially those containing alcohol) when cleaning the infant. Ointments or creams may help reduce friction and protect the baby's skin from irritation. Powders such as cornstarch or talc should be used cautiously, as they can be inhaled by the infant and may cause lung injury. If your baby has a yeast diaper rash, the health care provider will prescribe an antifungal cream to treat it. OTHER RASHES Heat rash or prickly heat is best treated by providing a cooler and less humid environment for the child. Powders are unlikely to help treat heat rash and should be stored out of reach of the infant to prevent accidental inhalation. Avoid ointments and creams because they tend to keep the skin warmer and block the pores. Erythema toxicum is normal in newborn babies and will go away on its own in a few days. You do not need to do anything for it. White or clear milia/miliaria will go away on their own. You do not need to do anything for it. For hives, talk with your provider to try to find the cause. Some causes require prescription medicines. Antihistamines may help stop the itching. BABY ACNE Normal washing is all that is necessary to treat baby acne most of the time. Use plain water or mild baby soap and only bathe your baby every 2 to 3 days. Avoid acne medicines used by adolescents and adults. CRADLE CAP For cradle cap, wash the hair or scalp with water or a mild baby shampoo. Use a brush to remove the flakes of dry skin. If this cannot be removed easily, apply an oil to the scalp to soften it. Cradle cap most often disappears by 18 months. If it does not disappear, it becomes infected, or if it is resistant to treatments, consult your provider. ECZEMA For skin problems caused by eczema, the keys to reducing rash are to reduce scratching and keep the skin moisturized.
While the majority of children with eczema will outgrow it, many will have sensitive skin as adults. When to Contact a Medical ProfessionalContact your child's provider if your child has:
What to Expect at Your Office VisitThe provider will perform a physical exam. The baby's skin will be thoroughly examined to determine the extent and type of the rash. Bring a list of all the products used on the child's skin. You may be asked questions such as:
Tests are seldom required but may include the following:
Depending on the cause of the rash, antihistamines may be recommended to decrease itching. Antibiotics may be prescribed if there is a bacterial infection. The provider may prescribe a cream for diaper rash caused by yeast. If the rash is severe and not caused by yeast, a corticosteroid cream may be recommended. For eczema, the provider may prescribe ointments or corticosteroid medicines to decrease inflammation. ReferencesBergqvist C, Ingen-Housz-Oro S, Chosidow O. Drug reactions. In: Bolognia JL, Schaffer JV, Cerroni L, eds. Dermatology. 5th ed. Philadelphia, PA: Elsevier Limited; 2025:chap 21. Haley A, Cummings K. Dermatology. In: Anderson CC, Kapoor S, Mark TE., eds. The Harriet Lane Handbook: The Johns Hopkins Hospital. 23rd ed. Philadelphia, PA: Elsevier; 2024:chap 8. Moon M, Guerrero AM, Li X, Koch E, Gehris RP. Dermatology. In: Zitelli BJ, McIntire SC, Nowalk AJ, Garrison J, eds. Zitelli and Davis' Atlas of Pediatric Physical Diagnosis. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 8. | ||
| ||
Review Date: 1/17/2025 Reviewed By: Charles I. Schwartz, MD, FAAP, Clinical Assistant Professor of Pediatrics, Perelman School of Medicine at the University of Pennsylvania, General Pediatrician at PennCare for Kids, Phoenixville, PA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


 Erythema toxicum o...
Erythema toxicum o... Heat rash
Heat rash Miliaria profunda ...
Miliaria profunda ...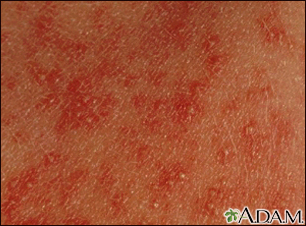 Erythema toxicum n...
Erythema toxicum n...