Knee scope - arthroscopic lateral retinacular release; Synovectomy - knee; Patellar (knee) debridement; Meniscus repair; Lateral release; Knee surgery; Meniscus - arthroscopy; Collateral ligament - arthroscopy DefinitionKnee arthroscopy is surgery that uses a tiny camera to look inside your knee. Small cuts are made to insert the camera and small surgical tools into your knee for the procedure. DescriptionThree different types of pain relief (anesthesia) may be used for knee arthroscopy surgery:
A cuff-like device may be put around your thigh to help control bleeding during the procedure. The surgeon will make 2 or 3 small cuts around your knee. Fluid (saline) will be pumped into your knee to inflate the knee. A narrow tube with a tiny camera on the end will be inserted through one of the cuts. The camera is attached to a video monitor that lets the surgeon see inside the knee. The surgeon may put other small surgical tools inside your knee through the other cuts. The surgeon will then fix or remove the problem in your knee. At the end of your surgery, the saline will be drained from your knee. The surgeon will close your cuts with sutures (stitches) and cover them with a dressing. Many surgeons take pictures of the procedure from the video monitor. You may be able to view these pictures after the operation so that you can see what was done. Why the Procedure Is PerformedArthroscopy may be recommended for these knee problems:
RisksThe risks of anesthesia and surgery are:
Additional risks of this surgery include:
Before the ProcedureDuring the 2 weeks before your surgery:
During the week before your surgery:
On the day of your surgery:
After the ProcedureYou will have an ace bandage on your knee over the dressing. Most people go home the same day they have surgery. Your provider will give you exercises to do that you can start after surgery. You may also be referred to a physical therapist. Outlook (Prognosis)Full recovery after knee arthroscopy will depend on what type of problem was treated. Problems such as a torn meniscus, broken cartilage, Baker cyst, and problems with the synovium are often easily fixed. Many people stay active after these surgeries. Recovery from simple procedures is fast in most cases. You may need to use crutches for a while after some types of surgery. Your provider may also prescribe pain medicine. Recovery will take longer if you have had a more complex procedure. If parts of your knee have been repaired or rebuilt, you may not be able to walk without crutches or a knee brace for several weeks. Full recovery may take several months to a year. If you also have arthritis in your knee, you will still have arthritis symptoms after surgery to repair other damage to your knee. ReferencesPhillips BB, Mihalko MJ. Arthroscopy of the lower extremity. In: Azar FM, Beaty JH, eds. Campbell's Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021:chap 51. Thompson SR, Miller MD. Basics of knee arthroscopy. In: Miller MD, Thompson SR, eds. DeLee Drez, & Miller's Orthopaedic Sports Medicine. 5th ed. Philadelphia, PA: Elsevier; 2020:chap 92. Waterman BR, Owens BD. Arthroscopic synovectomy and posterior knee arthroscopy. In: Miller MD, Browne JA, Cole BJ, Cosgarea AJ, Owens BD, eds. Operative Techniques: Knee Surgery. 2nd ed. Philadelphia, PA: Elsevier; 2018:chap 3. | ||
| ||
Review Date: 6/4/2025 Reviewed By: C. Benjamin Ma, MD, Professor, Chief, Sports Medicine and Shoulder Service, UCSF Department of Orthopaedic Surgery, San Francisco, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


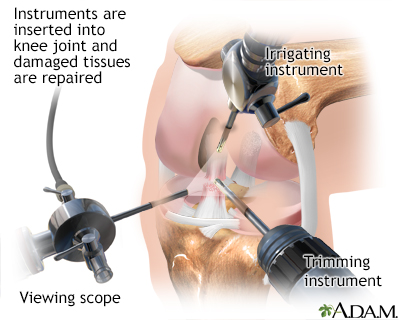 Knee arthroscopy
Knee arthroscopy