InformationInfant development is most often divided into the following areas:
PHYSICAL DEVELOPMENT An infant's physical development begins at the head, then moves to other parts of the body. For example, sucking comes before sitting, which comes before walking. Newborn to 2 months:
Primitive reflexes include:
3 to 4 months:
5 to 6 months:
6 to 9 months:
9 to 12 months:
SENSORY DEVELOPMENT
LANGUAGE DEVELOPMENT Crying is a very important way to communicate. By the baby's third day of life, mothers can tell their own baby's cry from that of other babies. By the first month of life, most parents can tell if their baby's cry means hunger, pain, or anger. Crying also causes a nursing mother's milk to fill the breast (letdown). The amount of crying in the first 3 months varies in a healthy infant, from 1 to 3 hours a day. Infants who cry more than 3 hours a day are often described as having colic. Colic in infants is rarely due to a problem with the body. In most cases, it stops by 4 months of age. Regardless of the cause, excessive crying needs a medical evaluation. It can cause family stress that can lead to child abuse. 0 to 2 months:
2 to 4 months:
4 to 6 months:
6 to 9 months:
9 to 12 months:
BEHAVIOR Newborn behavior is based on six states of consciousness:
Healthy babies with a normal nervous system can move smoothly from one state to another. Heart rate, breathing, muscle tone, and body movements are different in each state. Many bodily functions are not stable in the first months after birth. This is normal and differs from infant to infant. Stress and stimulation can affect: Periodic breathing, in which breathing starts and stops again, is normal. It is not a sign of sudden infant death syndrome sudden infant death syndrome (SIDS). Some infants will vomit or spit up after each feeding, but have nothing physically wrong with them. They continue to gain weight and develop normally. Other infants grunt and groan while making a bowel movement, but produce soft, blood-free stools, and their growth and feeding are good. This is due to immature abdominal muscles used for pushing and does not need to be treated. Sleep/wake cycles vary, and do not stabilize until a baby is 3 months old. These cycles occur in random intervals of 30 to 50 minutes at birth. Intervals gradually increase as the infant matures. By age 4 months, most infants will have one 5-hour period of uninterrupted sleep per day. Breast-fed infants will want to feed about every 2 hours. Formula-fed infants should be able to go 3 hours between feedings. During periods of rapid growth, they may feed more often. You do not need to give water to a baby. In fact, it could be dangerous. An infant who is drinking enough will produce 6 to 8 wet diapers in a 24-hour period. Teaching the infant to suck a pacifier or their own thumb provides comfort between feedings. SAFETY Safety is very important for infants. Base safety measures on the child's developmental stage. For example, around age 4 to 6 months, the infant may begin to roll over. Therefore, be very careful while the baby is on the changing table. Consider the following important safety tips:
CONTACT YOUR HEALTH CARE PROVIDER IF:
ReferencesOnigbanjo MT, Feigelman S. The first year. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 23. Hampton E, Olsson JM. The newborn. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 22. | ||
| ||
Review Date: 1/1/2025 Reviewed By: Charles I. Schwartz, MD, FAAP, Clinical Assistant Professor of Pediatrics, Perelman School of Medicine at the University of Pennsylvania, General Pediatrician at PennCare for Kids, Phoenixville, PA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


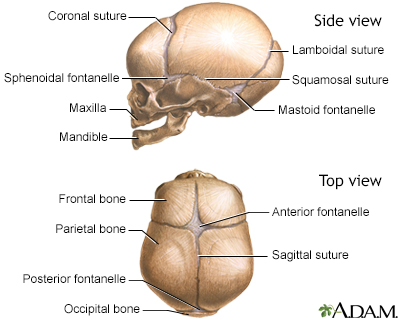 Skull of a newborn
Skull of a newborn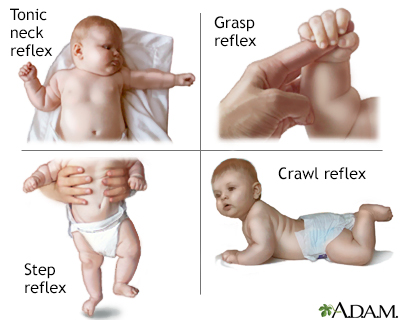 Infantile reflexes
Infantile reflexes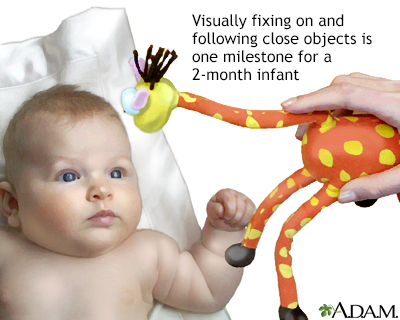 Developmental mile...
Developmental mile... Moro reflex
Moro reflex