Jaundice of the newborn; Neonatal hyperbilirubinemia; Bili lights - jaundice; Infant - yellow skin; Newborn - yellow skin DefinitionNewborn jaundice occurs when a baby has a high level of bilirubin in the blood. Bilirubin is a yellow substance that the body creates when it replaces old red blood cells. The liver helps break down the substance so it can be removed from the body in the stool. A high level of bilirubin makes a baby's skin and whites of the eyes look yellow. This is called jaundice. CausesIt is normal for a baby's bilirubin level to be a bit high after birth. When the baby is growing in the mother's womb (uterus), the placenta removes bilirubin from the baby's body. The placenta is the organ that grows during pregnancy to feed the baby. After birth, the baby's liver starts doing this job. But, it may take some time for the baby's liver to be able to do this efficiently. Most newborns have some jaundice. This is called physiological jaundice. It is usually noticeable when the baby is 2 to 4 days old. Most of the time, it does not cause problems and goes away within 2 weeks. Two types of jaundice may occur in newborns who are breastfed. Both types are usually harmless.
Severe newborn jaundice may occur if the baby has a condition that increases the number of red blood cells that need to be replaced in the body, such as:
Things that make it harder for the baby's body to remove bilirubin may also lead to more severe jaundice, including:
Babies who are born too early (premature) are more likely to develop jaundice than full-term babies. SymptomsJaundice causes a yellow color of the skin. It usually begins on the face and then moves down to the chest, belly area, legs, and soles of the feet. Sometimes, infants with severe jaundice may be very tired and feed poorly. Exams and TestsYour baby's health care providers will watch for signs of jaundice at the hospital. After the newborn goes home, family members will usually spot the jaundice. Any infant who appears jaundiced should have bilirubin levels measured right away. This can be done with a blood test. Many hospitals check total bilirubin levels on all babies at about 24 hours of age. Hospitals use probes that can estimate the bilirubin level just by touching the skin. High readings need to be confirmed with blood tests. Tests that will likely be done include: Further testing may be needed for babies who need treatment or whose total bilirubin level is rising more quickly than expected. TreatmentTreatment is not needed most of the time. When treatment is needed, the type will depend on:
A baby will need treatment if the bilirubin level is too high or is rising too quickly. A baby with jaundice needs to take in plenty of fluids with breast milk or formula:
Some newborns need to be treated before they leave the hospital. Others may need to go back to the hospital when they are a few days old. Treatment in the hospital usually lasts 1 to 2 days. Sometimes, special blue lights are used on infants whose bilirubin levels are very high. These lights work by helping to break down bilirubin in the skin. This is called phototherapy.
If the bilirubin level is not too high or is not rising quickly, you can do phototherapy at home with a fiberoptic blanket, which has tiny bright lights in it. You may also use a bed that shines light up from the mattress.
In the most severe cases of jaundice, an exchange transfusion is required. In this procedure, the baby's blood is replaced with fresh blood. Giving IV immunoglobulin to babies who have severe jaundice may also be effective in reducing bilirubin levels. Outlook (Prognosis)Newborn jaundice is not harmful most of the time. For most babies, jaundice will get better without treatment within 1 to 2 weeks. A very high level of bilirubin can damage the brain. This is called kernicterus. The condition is almost always diagnosed before the level becomes high enough to cause this damage. Treatment is usually effective. Possible ComplicationsRare, but serious complications from high bilirubin levels include:
When to Contact a Medical ProfessionalAll babies should be seen by a provider in the first 5 days of life to check for jaundice:
Jaundice is an emergency if the baby has a fever, has become listless, or is not feeding well. Jaundice may be dangerous in high-risk newborns. Jaundice is generally not dangerous in babies who were born full term and who do not have other medical problems. Contact the infant's provider if:
Talk with your baby's provider if you have questions. PreventionIn newborns, some degree of jaundice is normal and probably not preventable. The risk for serious jaundice can often be reduced by feeding babies at least 8 to 12 times a day for the first several days and by carefully identifying infants at highest risk. All pregnant women should be tested for blood type and unusual antibodies. If the mother is Rh negative, follow-up testing on the infant's umbilical cord is recommended. This may also be done if the mother's blood type is O positive. Careful monitoring of all babies during the first 5 days of life can prevent most complications of jaundice. This includes:
ReferencesKaplan M, Wong RJ, Bensen R, Sibley E, Stevenson DK. Neonatal jaundice and liver disease. In: Martin RJ, Fanaroff AA, eds. Fanaroff and Martin's Neonatal-Perinatal Medicine. 12th ed. Philadelphia, PA: Elsevier; 2025:chap 95. Kemper AR, Newman TB, Slaughter JL, et al. Clinical Practice Guideline Revision: Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics. 2022;150(3):e2022058859. PMID: 35927462 pubmed.ncbi.nlm.nih.gov/35927462/. Kliegman RM. Digestive system disorders. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 134. Rozance PJ, Wright CJ. The neonate. In: Landon MB, Galan HL, Jauniaux ERM, et al, eds. Gabbe's Obstetrics: Normal and Problem Pregnancies. 9th ed. Philadelphia, PA: Elsevier; 2025:chap 25. | ||
| ||
Review Date: 1/1/2025 Reviewed By: Charles I. Schwartz, MD, FAAP, Clinical Assistant Professor of Pediatrics, Perelman School of Medicine at the University of Pennsylvania, General Pediatrician at PennCare for Kids, Phoenixville, PA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


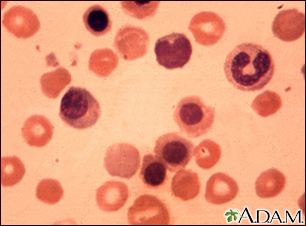 Erythroblastosis f...
Erythroblastosis f...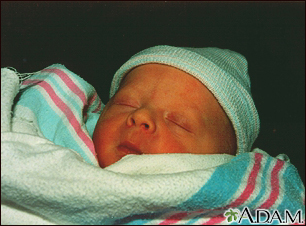 Jaundiced infant
Jaundiced infant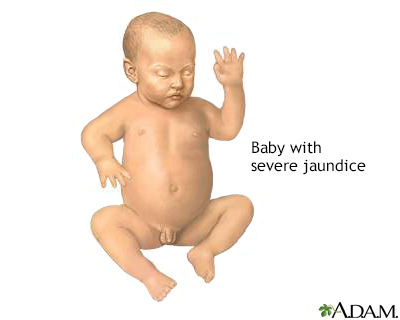 Infant jaundice
Infant jaundice