Overactive bladder; Detrusor instability; Detrusor hyperreflexia; Irritable bladder; Spasmodic bladder; Unstable bladder; Incontinence - urge; Bladder spasms; Urinary incontinence - urge DefinitionUrge incontinence occurs when you have a strong, sudden need to urinate that is difficult to delay. The bladder then squeezes, or spasms, and you may lose urine. CausesAs your bladder fills with urine from the kidneys, it stretches to make room for the urine. You should feel the first urge to urinate when there is a bit less than 1 cup (240 milliliters) of urine in your bladder. Most people can hold more than 2 cups (480 milliliters) of urine in the bladder. Two muscles help prevent the flow of urine:
When you urinate, the bladder wall muscle squeezes to force urine out of the bladder. As this happens, the sphincter muscle relaxes to allow the urine to pass through. All of these systems must work together to control urination:
The bladder may contract too often due to nervous system problems or bladder irritation. URGE INCONTINENCE With urge incontinence, you leak urine because the bladder muscles squeeze, or contract, at the wrong times. These contractions often occur no matter how much urine is in the bladder. Urge incontinence may result from:
In men, urge incontinence also may be due to:
In most cases of urge incontinence, no cause can be found. Although urge incontinence may occur in anyone at any age, it is more common in women and older adults. SymptomsSymptoms include:
Exams and TestsDuring a physical exam, your health care provider will look at your belly and rectum.
In most cases, the physical exam will not find any abnormalities. If there are nervous system causes, other problems also may be found. Tests may include the following:
TreatmentTreatment depends on how bad your symptoms are and how they affect your life. There are four main treatment approaches for urge incontinence:
BLADDER RETRAINING Managing urge incontinence most often begins with bladder retraining. This helps you become aware of when you lose urine because of bladder spasms. Then you relearn the skills you need to hold and release urine.
PELVIC FLOOR MUSCLE TRAINING Sometimes, Kegel exercises, biofeedback, or electrical stimulation may be used with bladder retraining. These methods help strengthen the muscles of your pelvic floor: Kegel exercises -- These are mainly used to treat people with stress incontinence. However, these exercises may also help relieve the symptoms of urge incontinence.
Vaginal cones -- This is a weighted cone that is inserted into the vagina to strengthen the pelvic floor muscles.
Biofeedback -- This method can help you learn to identify and control your pelvic floor muscles. It is usually managed by a specially trained physical therapist.
Electrical stimulation -- This uses a gentle electrical current to contract your bladder muscles.
Percutaneous tibial nerve stimulation (PTNS) -- This treatment may help some people with overactive bladder.
LIFESTYLE CHANGES Pay attention to how much water you drink and when you drink.
It also may help to stop consuming foods or drinks that may irritate the bladder, such as:
Avoid activities that irritate the urethra and bladder. This includes taking bubble baths or using harsh soaps. MEDICINES Medicines used to treat urge incontinence relax bladder contractions and help improve bladder function. There are several types of medicines that may be used alone or together:
These medicines may have side effects such as dizziness, constipation, or dry mouth. Talk with your provider if you notice bothersome side effects. If you have an infection, your provider will prescribe antibiotics. Be sure to take the entire amount as directed. SURGERY Surgery can help your bladder store more urine. It can also help relieve the pressure on your bladder. Surgery is used for people who do not respond to medicines or who have side effects associated with medicines. Sacral nerve stimulation involves implanting a small device under your skin. This device sends small electrical pulses to the sacral nerve (one of the nerves that comes out at the base of your spine). The electrical pulses can be adjusted to help relieve your symptoms. Augmentation cystoplasty is performed as a last resort for severe urge incontinence. In this surgery, a part of the bowel is added to the bladder. This increases the bladder size and allows it to store more urine. Possible complications include:
Urinary incontinence is a long-term (chronic) problem. While treatments can cure your condition, you should still see your provider to make sure you are doing well and check for possible problems. Outlook (Prognosis)How well you do depends on your symptoms, diagnosis, and treatment. Many people must try different treatments (some at the same time) to reduce symptoms. Getting better takes time, so try to be patient. A small number of people need surgery to control their symptoms. Possible ComplicationsPhysical complications are rare. The condition may get in the way of social activities, careers, and relationships. It can also make you feel bad about yourself. Rarely, this condition can cause severe increases in bladder pressure, which can lead to kidney damage. When to Contact a Medical ProfessionalContact your provider if:
PreventionStarting bladder retraining techniques early may help relieve your symptoms. ReferencesLentz GM, Miller JL. Lower urinary tract function and disorders: physiology of micturition, voiding dysfunction, urinary incontinence, urinary tract infections, and painful bladder syndrome. In: Gershenson DM, Lentz GM, Valea FA, Lobo RA, eds. Comprehensive Gynecology. 8th ed. Philadelphia, PA: Elsevier; 2022:chap 21. Lightner DJ, Gomelsky A, Souter L, Vasavada SP. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU Guideline Amendment 2019. J Urol. 2019;202(3):558-563. PMID: 31039103 pubmed.ncbi.nlm.nih.gov/31039103/. Newman DK, Burgio KL. Conservative management of urinary incontinence: behavioral and pelvic floor therapy, urethral and pelvic devices. In: Dmochowski RR, Kavoussi LR, Peters CA, et al, eds. Campbell-Walsh-Wein Urology. 13th ed. Philadelphia, PA: Elsevier; 2026:chap 114. Resnick NM, DuBeau CE. Urinary incontinence. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 115. Sebesta EM, Reynolds WS. Overactive bladder. In: Dmochowski RR, Kavoussi LR, Peters CA, et al, eds. Campbell-Walsh-Wein Urology. 13th ed. Philadelphia, PA: Elsevier; 2024:chap 110. | ||
| ||
Review Date: 7/1/2025 Reviewed By: Kelly L. Stratton, MD, FACS, Associate Professor, Department of Urology, University of Oklahoma Health Sciences Center, Oklahoma City, OK. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


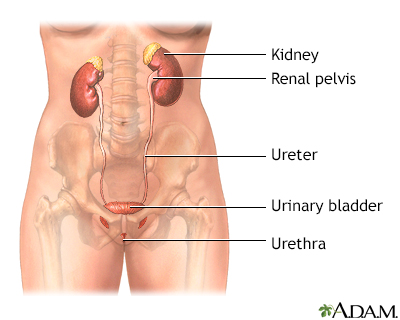 Female urinary tra...
Female urinary tra... Male urinary tract
Male urinary tract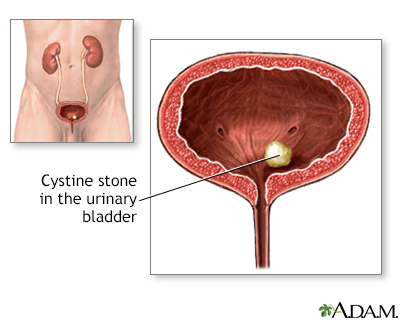 Cystinuria
Cystinuria