Spinal curvature; Infantile scoliosis; Juvenile scoliosis DefinitionScoliosis is an abnormal curving of the spine. Your spine is your backbone. It runs straight down your back. Everyone's spine naturally curves a bit. But people with scoliosis have a spine that curves too much. The spine might look like the letter C or S. CausesMost of the time, the cause of scoliosis is unknown. This is called idiopathic scoliosis. It is the most common type. It is grouped by age.
Scoliosis most often affects girls. Some people are more likely to have curving of the spine. Curving generally gets worse during a growth spurt. Other types of scoliosis are:
SymptomsMost often, there are no symptoms. If there are symptoms, they may include:
Exams and TestsYour health care provider will perform a physical exam. You will be asked to bend forward. This makes your spine easier to see. It may be hard to see changes in the early stages of scoliosis. The exam may show:
X-rays of the spine are done. X-rays are important because the actual curving of the spine may be worse than what your doctor can see during an exam. Other tests may include:
TreatmentTreatment depends on many things:
Most people with idiopathic scoliosis do not need treatment. But you should still be checked by your provider about every 6 months. If you are still growing, your provider might recommend a back brace. A back brace prevents further curving. There are many different types of braces. What kind you get depends on the size and location of your curve. Your provider will pick the best one for you and show you how to use it. Back braces can be adjusted as you grow. Back braces work best in people over age 10 with continued growing potential. Braces do not work for those with congenital or neuromuscular scoliosis. You may need surgery if the spine curve is severe or getting worse very quickly. Surgery involves correcting the curve as much as possible:
Scoliosis treatment may also include:
Support GroupsSeek support and more information from organizations that specialize in scoliosis. Outlook (Prognosis)How well a person with scoliosis does depends on the type, cause, and severity of the curve. The more severe the curving, the more likely it will get worse after the child stops growing. People with mild scoliosis do well with braces. They usually do not have long-term problems. Back pain may be more likely when the person gets older. The outlook for those with neuromuscular or congenital scoliosis varies. They may have another serious disorder, such as cerebral palsy or muscular dystrophy, so their goals of treatment may be much different. Often, the goal of surgery is simply to allow a child to be able to walk more properly or sit upright in a wheelchair. Congenital scoliosis is difficult to treat and usually requires many surgeries. Possible ComplicationsComplications of scoliosis can include:
When to Contact a Medical ProfessionalContact your provider if you suspect your child may have scoliosis. PreventionRoutine scoliosis screening is now done in middle schools. Such screening has helped detect early scoliosis in many children. Back and abdominal muscle strengthening can help stabilize the curvature. ReferencesBuell TJ, Lark R, Smith JS, Shaffrey CI. An approach for treatment of complex pediatric spinal deformity. In: Steinmetz MP, Berven SH, Benzel EC, eds. Benzel's Spine Surgery: Techniques, Complication Avoidance, and Management. 5th ed. Philadelphia, PA: Elsevier; 2022:chap 143. Mistovich RJ, Spiegel DA. The spine. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 699. Negrini S, Di Felice F, Donzelli S, Zaina F. Scoliosis and kyphosis. In: Frontera WR, Silver JK, Rizzo TD Jr, eds. Essentials of Physical Medicine and Rehabilitation: Musculoskeletal Disorders, Pain, and Rehabilitation. 4th ed. Philadelphia, PA: Elsevier; 2019:chap 153. | ||
| ||
Review Date: 8/12/2023 Reviewed By: C. Benjamin Ma, MD, Professor, Chief, Sports Medicine and Shoulder Service, UCSF Department of Orthopaedic Surgery, San Francisco, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


 Scoliosis
Scoliosis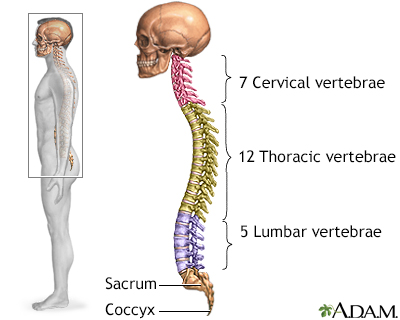 Skeletal spine
Skeletal spine Scoliosis
Scoliosis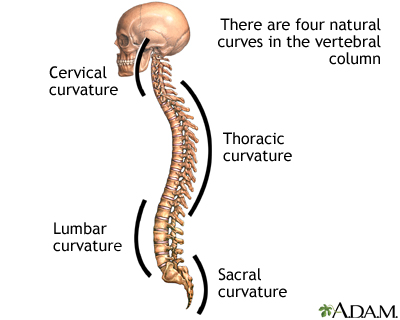 Spinal curves
Spinal curves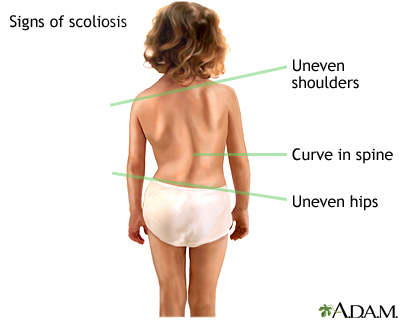 Signs of scoliosis
Signs of scoliosis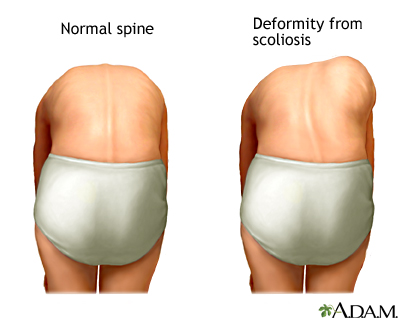 Forward bend test
Forward bend test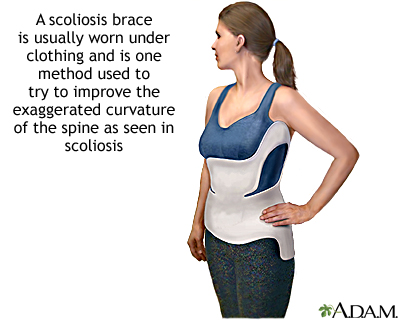 Scoliosis brace
Scoliosis brace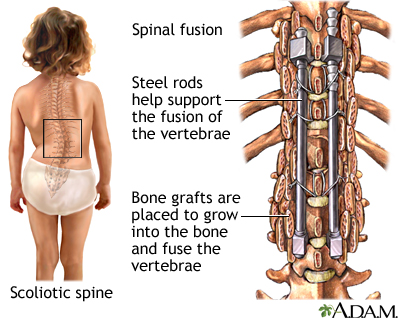 Spinal fusion
Spinal fusion