Enlarged parathyroid glands; Osteoporosis - parathyroid hyperplasia; Bone thinning - parathyroid hyperplasia; Osteopenia - parathyroid hyperplasia; High calcium level - parathyroid hyperplasia; Chronic kidney disease - parathyroid hyperplasia; Kidney failure - parathyroid hyperplasia; Overactive parathyroid - parathyroid hyperplasia DefinitionParathyroid hyperplasia is the enlargement of all 4 parathyroid glands. The parathyroid glands are located in the neck, near or attached to the back side of the thyroid gland. CausesThe parathyroid glands help regulate calcium absorption, use, and removal by the body. They do this by producing parathyroid hormone (PTH). PTH helps regulate calcium, phosphorus, and vitamin D levels in the blood and bone. It is important for healthy bones. Parathyroid hyperplasia may occur in people without a family history of the disease, or as part of 3 inherited syndromes:
In people with an inherited syndrome, a changed (variant) gene is passed down through the family. You only need to get the gene from one parent to develop the condition.
Parathyroid hyperplasia that isn't part of an inherited syndrome is much more common. It occurs due to other medical conditions. The most common conditions that can cause parathyroid hyperplasia are chronic kidney disease and chronic vitamin D deficiency. In both cases, the parathyroid glands become enlarged because vitamin D and calcium levels are too low. SymptomsSymptoms may include:
Exams and TestsBlood tests will be done to check levels of:
Other tests include:
TreatmentIf parathyroid hyperplasia is due to kidney disease or low vitamin D level and it is found early, your health care provider may recommend that you take vitamin D, vitamin D-like medicines, and other medicines. Surgery is usually done when the parathyroid glands are producing too much PTH and causing symptoms. Usually 3 1/2 glands are removed. The remaining tissue may be implanted in the forearm or neck muscle. This allows easy access to the tissue if symptoms come back. This tissue is implanted to prevent the body from having too little PTH, which can result in low calcium levels (from hypoparathyroidism). Outlook (Prognosis)After surgery, a high blood calcium level may persist or return. Surgery can sometimes cause hypoparathyroidism, which makes blood calcium level too low. Possible ComplicationsParathyroid hyperplasia can cause hyperparathyroidism, which leads to an increase in blood calcium level. Complications include increased calcium in the kidneys, which can cause kidney stones, and osteitis fibrosa cystica (a softened, weak area in the bones). Surgery can sometimes damage the nerves that control the vocal cords. This can affect the strength of your voice. Complications may result from the other tumors that are part of the MEN syndromes. When to Contact a Medical ProfessionalContact your provider if:
PreventionIf you have a family history of the MEN syndromes, you may want to have genetic screening to check for the variant gene. Those who have the variant gene may have routine screening tests to detect any early symptoms. ReferencesReid LM, Kamani D, Randolph GW. Management of parathyroid disorders. In: Flint PW, Francis HW, Haughey BH, et al, eds. Cummings Otolaryngology: Head and Neck Surgery. 7th ed. Philadelphia, PA: Elsevier; 2021:chap 123. Thakker RV. The parathyroid glands, hypercalcemia and hypocalcemia. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 227. Walker MD, Bilezikian JP. Primary hyperparathyroidism. In: Robertson RP, ed. DeGroot's Endocrinology. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 54. | ||
| ||
Review Date: 5/20/2024 Reviewed By: Sandeep K. Dhaliwal, MD, board-certified in Diabetes, Endocrinology, and Metabolism, Springfield, VA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


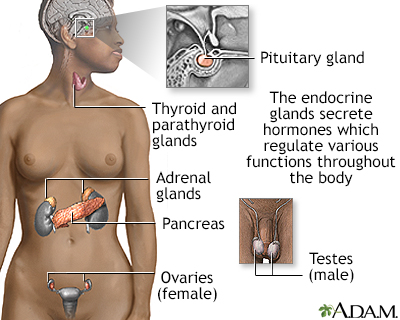 Endocrine glands
Endocrine glands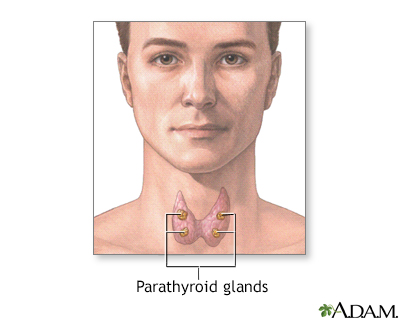 Parathyroid glands
Parathyroid glands