Pituitary dwarfism; Acquired growth hormone deficiency; Isolated growth hormone deficiency; Congenital growth hormone deficiency; Panhypopituitarism; Short stature - growth hormone deficiency DefinitionGrowth hormone deficiency means the pituitary gland does not make enough growth hormone. CausesThe pituitary gland is located at the base of the brain. This gland controls the body's balance of hormones. It also makes growth hormone. This hormone causes a child to grow. Growth hormone deficiency may be present at birth. Growth hormone deficiency may be the result of a medical condition. Severe brain injury may also cause growth hormone deficiency. Children with physical defects of the face and skull, such as cleft lip or cleft palate, may have decreased growth hormone level. Most of the time, the cause of growth hormone deficiency is unknown. SymptomsSlow growth may first be noticed in infancy and continue through childhood. Your child's health care provider will most often draw your child's growth curve on a growth chart. Children with growth hormone deficiency have a slow or flat rate of growth. The slow growth may not show up until a child is 2 or 3 years old. The child will be much shorter than most children of the same age and sex. The child will still have normal body proportions, but may be chubby. The child's face often looks younger than other children of the same age. The child will have normal intelligence in most cases. In older children, puberty may come late or may not come at all, depending on the cause. Exams and TestsA physical exam, including weight, height, and body proportions, will show signs of slowed growth. The child will not follow the normal growth curves. A hand x-ray can determine bone age. Normally, the size and shape of bones change as a person grows. These changes can be seen on an x-ray and they most often follow a pattern as a child grows older. Testing is most often done after the provider has looked into other causes of poor growth. Tests that may be done include:
TreatmentTreatment involves growth hormone shots (injections) given at home. The shots are most often given once a day. Older children can often learn how to give themselves the shot. Treatment with growth hormone is long-term, often lasting for several years. During this time, the child needs to be seen regularly by their provider to ensure the treatment is working. If needed, the provider will change the dosage of the medicine. Serious side effects of growth hormone treatment are rare. Common side effects include:
Outlook (Prognosis)The earlier the condition is treated, the better the chance that a child will grow to near-normal adult height. Many children gain 4 or more inches (about 10 centimeters) during the first year, and 3 or more inches (about 7.6 centimeters) during the next 2 years. The rate of growth then slowly decreases. Growth hormone therapy does not work for all children. Left untreated, growth hormone deficiency may lead to short stature and delayed puberty. Growth hormone deficiency can occur with deficiencies of other hormones such as those that control:
When to Contact a Medical ProfessionalContact your provider if your child seems abnormally short for their age. PreventionMost cases are not preventable. Review your child's growth chart with your child's provider at each checkup. If there is concern about your child's growth rate, evaluation by a specialist is recommended. ReferencesCooke DW, Divall SA, Radovick S. Normal and aberrant growth in children. In: Melmed S, Auchus RJ, Goldfine AB, Koenig RJ, Rosen CJ, eds. Williams Textbook of Endocrinology. 14th ed. Philadelphia, PA: Elsevier; 2020:chap 25. Patterson BC, Felner EI. Hypopituitarism. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 573. Weiss RE. Anterior pituitary. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 205. | ||
| ||
Review Date: 8/5/2023 Reviewed By: Neil K. Kaneshiro, MD, MHA, Clinical Professor of Pediatrics, University of Washington School of Medicine, Seattle, WA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


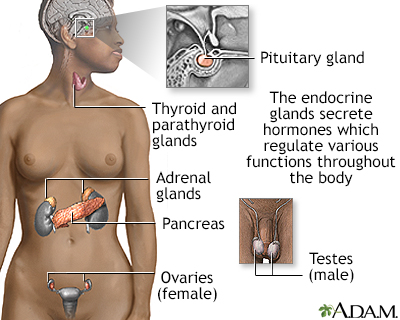 Endocrine glands
Endocrine glands Height/weight char
Height/weight char