VSD; Interventricular septal defect; Congenital heart defect - VSD DefinitionA ventricular septal defect is a hole in the wall that separates the right and left ventricles of the heart. Ventricular septal defect is one of the most common congenital (present from birth) heart defects. It occurs in nearly half of all children with congenital heart disease. It may occur by itself or with other congenital diseases. CausesBefore a baby is born, the right and left ventricles of the heart are not separate. As the fetus grows, a septum (wall) forms to separate these 2 ventricles. If the wall does not completely form, a hole remains. This hole is known as a ventricular septal defect, or a VSD. The hole can occur in different locations along the septal wall. There can be a single hole or multiple holes. VSD is a common congenital heart defect. The baby may have no symptoms and the hole can close over time as the wall continues to grow after birth. If the hole is large, too much blood will be pumped to the lungs. This can lead to heart failure. If the hole is small, it may not be detected for years and only discovered in adulthood. The cause of VSD is not yet known. This defect often occurs along with other congenital heart defects. In adults, VSDs can be rare, but serious, complication of heart attacks. These holes do not result from a birth defect. SymptomsPeople with VSDs may not have symptoms. However, if the hole is large, the baby often has symptoms related to heart failure. The most common symptoms include:
Exams and TestsListening with a stethoscope most often reveals a heart murmur. The loudness of the murmur is related to the size of the defect and amount of blood crossing the defect. Tests may include:
TreatmentIf the defect is small, no treatment may be needed. But the baby should be closely monitored by a heart specialist (cardiologist). This is to make sure that the hole eventually closes properly, and signs of heart failure do not occur. Babies with a large VSD who have symptoms related to heart failure may need medicine to control the symptoms and surgery to close the hole. Diuretic medicines are often used to relieve symptoms of congestive heart failure. If symptoms continue, even with medicine, surgery to close the defect with a patch is needed. Some VSDs can be closed with a special device during a cardiac catheterization, which avoids the need for surgery. This is called transcatheter closure. However, only certain types of defects can successfully be treated this way. Having surgery for a VSD with no symptoms is controversial, especially when there is no evidence of heart damage. Discuss this carefully with your child's provider. Outlook (Prognosis)Many small defects will close on their own. Surgery can repair defects that do not close. In most cases, a person will not have any ongoing medical issues related to the defect if it is closed with surgery or closes on its own. Complications may occur if a large defect is not treated and there is permanent damage to the lungs. Possible ComplicationsComplications may include:
When to Contact a Medical ProfessionalMost often, this condition is diagnosed during a routine exam of an infant. Contact your infant's provider if the baby seems to be having trouble breathing, or if the baby seems to have an unusual number of respiratory infections. PreventionExcept for a VSD that is caused by a heart attack, this condition is always present at birth. Drinking alcohol and using the antiseizure medicines valproic acid (Depakote) and phenytoin (Dilantin) during pregnancy may increase the risk for VSDs. Other than avoiding these things during pregnancy, there is no known way to prevent a VSD. Women who plan to become pregnant should be immunized against rubella if they are not already immune. Rubella infection in a pregnant woman can cause congenital heart disease. Women who are pregnant should get good prenatal care:
ReferencesBernstein D. Evaluation and screening of the infant or child with congenital heart disease. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 474. Valente AM, Dorfman AL, Babu-Narayan SV, Kreiger EV. Congenital heart disease in the adolescent and adult. In: Libby P, Bonow RO, Mann DL, Tomaselli GF, Bhatt DL, Solomon SD, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 12th ed. Philadelphia, PA: Elsevier; 2022:chap 82. Well A, Fraser CD. Congenital heart disease. In: Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 21st ed. St Louis, MO: Elsevier; 2022:chap 59. | ||
| ||
Review Date: 10/1/2025 Reviewed By: Thomas S. Metkus MD, PhD, Associate Professor of Medicine and Surgery, Johns Hopkins University School of Medicine, Baltimore, MD. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


 Heart - section th...
Heart - section th... Heart - front view
Heart - front view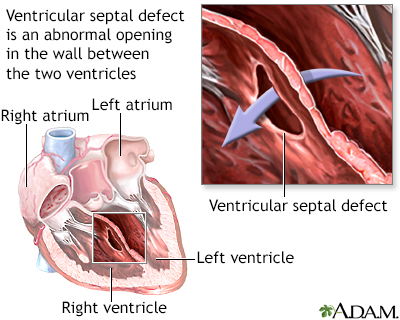 Ventricular septal...
Ventricular septal...