Birth defect - gastroschisis; Abdominal wall defect - infant; Abdominal wall defect - neonate; Abdominal wall defect - newborn DefinitionGastroschisis is a birth defect in which an infant's intestines are outside of the body because of a hole in the abdominal wall. CausesBabies with gastroschisis are born with a hole in the abdominal wall. The child's intestines often stick out (protrude) through the hole. The condition looks similar to an omphalocele. An omphalocele, however, is a birth defect in which the infant's intestine or other abdominal organs protrude through a hole in the belly button area and are covered with a membrane. With gastroschisis, there is no covering membrane. Abdominal wall defects develop as a baby grows inside the mother's womb. During development, the intestine and other organs (liver, bladder, stomach, and ovaries, or testes) develop outside the body at first and then usually return inside. In babies with gastroschisis, the intestines (and sometimes the stomach) remain outside the abdominal wall, without a membrane covering them. The exact cause of abdominal wall defects is not known. Mothers with the following may be at higher risk of having babies with gastroschisis:
Babies with gastroschisis usually do not have other related birth defects. SymptomsA gastroschisis is usually seen during a prenatal ultrasound. It can also be seen when the baby is born. There is a hole in the abdominal wall. The small intestine is often outside the abdomen near the umbilical cord. Other organs that may also be outside the abdomen are the large intestine, stomach, and/or gallbladder. Usually the intestine is irritated by the exposure to amniotic fluid. The baby may have problems absorbing food. Exams and TestsPrenatal ultrasounds often identify infants with gastroschisis before birth, usually by 20 weeks of pregnancy. TreatmentIf gastroschisis is found before birth, the mother will need special monitoring to make sure her unborn baby remains healthy. Treatment for gastroschisis involves surgery. Usually the infant's abdominal cavity is too small for the intestine to fit back in at birth. So, a mesh sack is stitched around the borders of the defect and the edges of the defect are pulled up. The sack is called a silo. Over the next week or two, the intestine returns into the abdominal cavity and the defect can then be closed. The baby's temperature must be carefully controlled, because the exposed intestine allows body heat to escape. Because of the pressure involved in returning the intestines to the abdomen, the baby may need breathing support with a ventilator. Other treatments for the baby include nutrients by IV and antibiotics to prevent infection. Even after the defect is closed, IV nutrition will continue as milk feedings must be introduced slowly. Outlook (Prognosis)The baby has a good chance of recovering if there are no other problems and if the abdominal cavity is large enough. A very small abdominal cavity may result in complications that require more surgeries. Plans should be made for careful delivery and immediate management of the problem after birth. The baby should be delivered in a medical center that is skilled at repairing abdominal wall defects. Babies are likely to do better if they do not need to be taken to another center for further treatment. Possible ComplicationsBecause of the exposure to amniotic fluid, babies' intestines may not work normally even after the organs are put back inside the abdominal cavity. Babies with gastroschisis need time for their intestines to recover and become used to taking feedings. A small number of babies with gastroschisis (about 10 to 20%) may have intestinal atresia (parts of the intestines that did not develop in the womb). These babies require further surgery to relieve obstruction. The increased pressure from the misplaced abdominal contents can decrease blood flow to the intestines and kidneys and cause more long-term damage. It can also make it difficult for the baby to expand the lungs, leading to breathing problems. Another possible complication is bowel death leading to necrosis of the bowel. This occurs when intestinal tissue dies due to low blood flow or infection. This risk may be reduced in babies who receive breast milk rather than formula. This condition (gastroschisis) is apparent at birth and will be detected in the hospital at delivery if it has not already been seen on routine fetal ultrasound exams during pregnancy. If you have given birth at home and your baby appears to have this defect, call 911 or the local emergency number right away. When to Contact a Medical ProfessionalThis problem is diagnosed and treated in the hospital right after birth. After returning home, contact your health care provider if your baby develops any of these symptoms:
ReferencesCenters for Disease Control and Prevention website. Birth defects. Gastroschisis. www.cdc.gov/birth-defects/about/gastroschisis.html. Updated May 16, 2024. Accessed June 18, 2024. Islam S. Congenital abdominal wall defects: gastroschisis and omphalocele. In: Holcomb GW, Murphy JP, St. Peter SD, eds. Holcomb and Ashcraft's Pediatric Surgery. 7th ed. Philadelphia, PA: Elsevier; 2020:chap 48. Polites S, Nathan JD. Newborn abdominal wall defects. In: Wyllie R, Hyams JS, Kay M, eds. Pediatric Gastrointestinal and Liver Disease. 6th ed. Philadelphia, PA: Elsevier; 2021:chap 58. | ||
| ||
Review Date: 12/31/2023 Reviewed By: Mary J. Terrell, MD, IBCLC, Neonatologist, Cape Fear Valley Medical Center, Fayetteville, NC. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


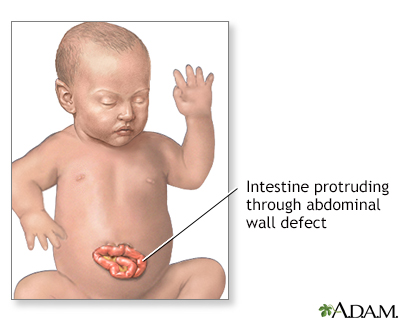 Infant abdominal h...
Infant abdominal h...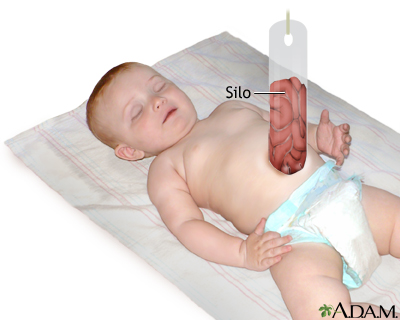 Silo
Silo