Pediatric asthma; Asthma - pediatric; Wheezing - asthma - children DefinitionAsthma is a disease that causes the airways to swell and get narrow. It leads to wheezing, shortness of breath, chest tightness, and coughing. CausesAsthma is caused by swelling (inflammation) in the airways. During an asthma attack, the muscles surrounding the airways tighten. The lining of the air passages swells. As a result, less air is able to pass through. Asthma is often seen in children. It is a leading cause of missed school days and hospital visits for children. An allergic reaction is a key part of asthma in children. Asthma and allergies often occur together. In children who have sensitive airways, asthma symptoms can be triggered by breathing in substances called allergens, or triggers. Common asthma triggers include:
SymptomsBreathing problems are common. They can include:
When your child is having a hard time breathing, the skin of their chest and neck may suck inward (chest or neck retractions). Other symptoms of asthma in children include:
Your child's asthma symptoms may vary. Symptoms may appear often or develop only when triggers are present. Some children are more likely to have asthma symptoms at night. Exams and TestsYour health care provider will use a stethoscope to listen to your child's lungs. Your provider may be able to hear asthma sounds. However, lung sounds are often normal when your child is not having an asthma attack. Your provider will have your child breathe into a device called a peak flow meter. Peak flow meters can tell how well they can blow air out of their lungs. If the airways are narrow due to asthma, peak flow values drop. You and your child will learn to measure peak flow at home. Your child's provider may order the following tests:
TreatmentYou and your child's providers should work together as a team to create and carry out an asthma action plan. This plan will tell you how to:
The plan should also tell you when to contact your child's provider. It is important to know what questions to ask your child's provider. Children with asthma may need a lot of support at school.
ASTHMA MEDICINES There are two basic kinds of medicine used to treat asthma. Long-term control medicines are taken every day to prevent asthma symptoms. Your child should take these medicines even if no symptoms are present. Some children may need more than one long-term control medicine. Types of long-term control medicines include:
Quick relief or rescue asthma medicines work fast to control asthma symptoms. Children take them when they are coughing, wheezing, having trouble breathing, or having an asthma attack. Some of your child's asthma medicines can be taken using an inhaler.
GETTING RID OF TRIGGERS It is important to know your child's asthma triggers. Avoiding them is the first step toward helping your child feel better. Keep pets away from your child's bedroom. No one should smoke in a house or around a child with asthma.
Keep the house clean. Keep food in containers and out of bedrooms. This helps reduce the possibility of cockroaches, which can trigger asthma attacks. Cleaning products in the home should be unscented. MONITOR YOUR CHILD'S ASTHMA Checking peak flow is one of the best ways to monitor and control asthma. It can help you keep your child's asthma from getting worse. Asthma attacks usually do not happen without warning. Children under age 5 may not be able to use a peak flow meter well enough for it to be helpful. However, a child should start using the peak flow meter at a young age to get used to it. An adult should always watch for a child's asthma symptoms. Outlook (Prognosis)With proper treatment, most children with asthma can live a normal life. When asthma is not well controlled, it can lead to missed school, problems playing sports, missed work for parents, and many visits to the provider's office and emergency room. Asthma symptoms often lessen or go away completely as the child gets older. Asthma that is not well controlled can lead to lasting lung problems. In rare cases, asthma is a life-threatening disease. Families need to work closely with their providers to develop a plan to care for a child with asthma. When to Contact a Medical ProfessionalContact your child's provider if you think your child has new symptoms of asthma. If your child has been newly diagnosed with asthma, contact their provider:
If your child is having trouble breathing or having an asthma attack, get medical help right away. Emergency symptoms include:
A child who is having a severe asthma attack may need to stay in the hospital and get oxygen and medicines through a vein (intravenous line or IV). ReferencesJackson DJ, Lemanske RF, Bacharier LB. Management of asthma in infants and children. In: Burks AW, Holgate ST, O'Hehir RE, et al, eds. Middleton's Allergy: Principles and Practice. 9th ed. Philadelphia, PA: Elsevier; 2020:chap 50. Liu AH, Bacharier LB, Fitzpatrick AM, Sicherer SH. Childhood asthma. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 185. Lugogo N, Que LG, Carr TF, Kraft M. Asthma: diagnosis and management. In: Broaddus VC, Ernst JD, King TE, et al, eds. Murray & Nadel's Textbook of Respiratory Medicine. 7th ed. Philadelphia, PA: Elsevier; 2022:chap 62. National Heart, Lung, and Blood Institute website. 2020 Focused Updates to the Asthma Management Guidelines: A Report from the National Asthma Education and Prevention Program Coordinating Committee Expert Panel Working Group. www.nhlbi.nih.gov/resources/2020-focused-updates-asthma-management-guidelines. Updated December 2020. Accessed July 14, 2025. | ||
| ||
Review Date: 4/6/2025 Reviewed By: Neil K. Kaneshiro, MD, MHA, Clinical Professor of Pediatrics, University of Washington School of Medicine, Seattle, WA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


 Normal versus asth...
Normal versus asth...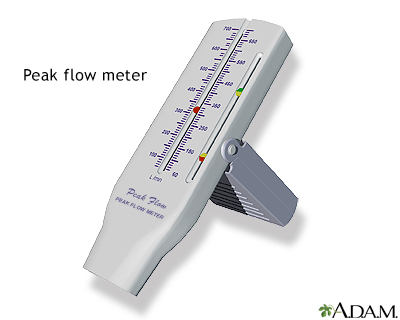 Peak flow meter
Peak flow meter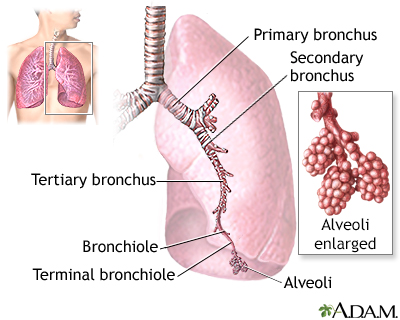 Lungs
Lungs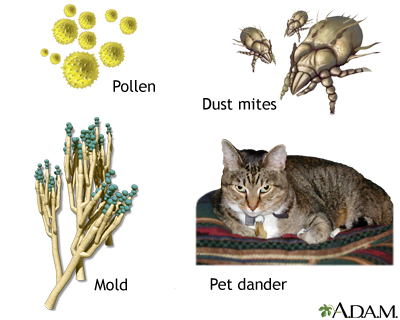 Common asthma trig...
Common asthma trig...