Seizure - fever induced; Febrile convulsions DefinitionA febrile seizure is a convulsion in a child triggered by a fever. CausesA temperature of 100.4°F (38°C) or above may cause febrile seizures in children. A febrile seizure can be frightening for any parent or caregiver. Most of the time, a febrile seizure does not cause any harm. The child usually does not have a more serious long-term health problem. Febrile seizures occur most often in otherwise healthy children between ages 6 months and 5 years. Toddlers are most commonly affected. Febrile seizures often run in families. Most febrile seizures occur in the first 24 hours of an illness. It may not occur when the fever is highest. A cold or viral illness may trigger a febrile seizure. SymptomsA febrile seizure may be as mild as the child's eyes rolling or limbs stiffening. A simple febrile seizure stops by itself within a few seconds to 10 minutes. It is often followed by a brief period of drowsiness or confusion. Symptoms may include any of the following:
A seizure lasting longer than 15 minutes, is in just one part of the body, or that occurs again during the same illness is not a normal febrile seizure. The health care provider may diagnose febrile seizure if the child has a tonic-clonic seizure but does not have a history of seizure disorders (epilepsy). A tonic-clonic seizure involves the entire body. In infants and young children, it is important to rule out other causes of a first-time seizure, especially meningitis (bacterial infection of the covering of the brain and spinal cord). Exams and TestsWith a typical febrile seizure, the examination usually is normal, other than symptoms of the illness causing the fever. Often, the child will not need a full seizure workup, which includes an EEG, head CT, and lumbar puncture (spinal tap). Further testing may be needed if the child:
TreatmentThe aim of treatment is to manage the underlying cause. The following measures help keep the child safe during a seizure:
If the seizure lasts several minutes, call 911 or the local emergency number to have an ambulance take your child to the hospital. Contact your child's provider as soon as possible to describe your child's seizure. After the seizure, the most important step is to identify the cause of the fever. The focus is on bringing the fever down. The provider may tell you to give your child medicines to reduce the fever. Follow instructions exactly on how much and how often to give your child the medicine. These medicines, however, do not reduce the chance of having febrile seizures in the future. It is normal for children to sleep or be drowsy or confused for a short time right after a seizure. Outlook (Prognosis)The first febrile seizure can be frightening for parents. Most parents are afraid that their child will die or have brain damage. However, simple febrile seizures are harmless. There is no evidence that they cause death, brain damage, epilepsy, or learning problems. Most children outgrow febrile seizures by age 5. Few children have more than 3 febrile seizures in their lifetime. The number of febrile seizures is not related to future risk for epilepsy. Children who would develop epilepsy anyway will sometimes have their first seizures during fevers. These seizures most often do not appear like a typical febrile seizure. When to Contact a Medical ProfessionalIf the seizure lasts several minutes, call 911 or the local emergency number to have an ambulance bring your child to the hospital. If the seizure ends quickly, drive the child to an emergency room when it is over. Take your child to their provider if:
Contact their provider if other symptoms occur before or after the seizure, such as:
PreventionBecause febrile seizures can be the first sign of illness, it is often not possible to prevent them. A febrile seizure does not mean that your child is not getting the proper care. Occasionally, a provider will prescribe a medicine called diazepam to prevent or treat febrile seizures that occur more than once. However, no drug is completely effective in preventing febrile seizures. ReferencesAbou-Khalil BW, Gallagher MJ, Macdonald RL. Epilepsies. In: Jankovic J, Mazziotta JC, Pomeroy SL, Newman NJ, eds. Bradley and Daroff's Neurology in Clinical Practice. 8th ed. Philadelphia, PA: Elsevier; 2022:chap 100. Mick NW. Pediatric fever. In: Walls RM, ed. Rosen's Emergency Medicine: Concepts and Clinical Practice. 10th ed. Philadelphia, PA: Elsevier; 2023:chap 161. Mikati MA, Tchapyjnikov D. Seizures in childhood. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 611. National Institute of Neurological Disorders and Stroke website. Febrile seizures. www.ninds.nih.gov/health-information/disorders/febrile-seizures. Updated July 19, 2024. Accessed September 8, 2024. Seinfeld S, Shinnar S. Febrile seizures. In: Swaiman KF, Ashwal S, Ferriero DM, et al, eds. Swaiman's Pediatric Neurology: Principles and Practice. 6th ed. Philadelphia, PA: Elsevier; 2017:chap 65. | ||
| ||
Review Date: 2/17/2024 Reviewed By: Charles I. Schwartz, MD, FAAP, Clinical Assistant Professor of Pediatrics, Perelman School of Medicine at the University of Pennsylvania, General Pediatrician at PennCare for Kids, Phoenixville, PA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. Editorial update 09/08/2024. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


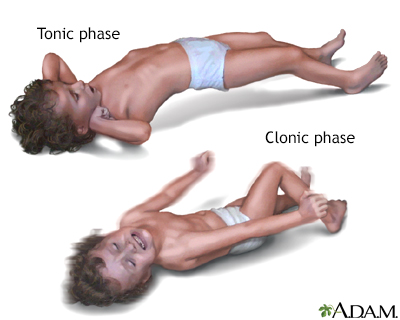 Grand mal seizure
Grand mal seizure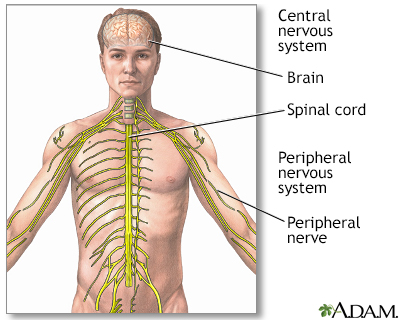 Central nervous sy...
Central nervous sy...