Incontinence - stress; Bladder incontinence stress; Pelvic prolapse - stress incontinence; Stress incontinence; Leakage of urine - stress incontinence; Urinary leakage - stress incontinence; Pelvic floor - stress incontinence DefinitionStress urinary incontinence occurs when your bladder leaks urine during physical activity or exertion. It may happen when you cough, sneeze, lift something heavy, change positions, or exercise. CausesStress incontinence occurs when the tissue that supports your urethra gets weak.
When either set of muscles become weak, urine can pass when pressure is placed on your bladder. You may notice it when you:
Weakened pelvic floor muscles may be caused by:
Stress incontinence is common in women. Some things increase your risk, such as:
SymptomsThe main symptom of stress incontinence is leaking urine when you:
Exams and TestsYour health care provider will perform a physical exam. This will include:
Tests may include:
TreatmentTreatment depends on how your symptoms affect your life. There are 3 types of treatment for stress incontinence:
There are no medicines for treatment of stress incontinence. Some providers may prescribe a medicine called duloxetine. This medicine is not approved by FDA for the treatment of stress incontinence. BEHAVIOR CHANGES Making these changes may help:
BLADDER TRAINING Bladder training may help you control your bladder. You will be asked to urinate at regular intervals. Slowly, the time interval is increased. This causes the bladder to stretch and hold more urine. PELVIC FLOOR MUSCLE TRAINING There are different ways to strengthen the muscles in your pelvic floor.
SURGERIES If other treatments do not work, your provider may suggest surgery. Surgery may help if you have bothersome stress incontinence. Most providers suggest surgery only after trying nonsurgical treatments.
Outlook (Prognosis)Getting better takes time, so try to be patient. Symptoms most often get better with nonsurgical treatments. However, they will not cure stress incontinence. Surgery can cure most people of stress incontinence. Treatment does not work as well if you have:
Possible ComplicationsPhysical complications are rare and most often mild. They can include:
The condition may get in the way of social activities, careers, and relationships. It also may lead to:
Complications associated with surgery include:
When to Contact a Medical ProfessionalContact your provider if you have symptoms of stress incontinence and they bother you. PreventionDoing Kegel exercises may help prevent symptoms. Women may want to do Kegels during and after pregnancy to help prevent incontinence. ReferencesAl-Mousa RT, Hashim H. Evaluation and management of men with urinary incontinence. In: Partin AW, Dmochowski RR, Kavoussi LR, Peters CA, eds. Campbell-Walsh-Wein Urology. 12th ed. Philadelphia, PA: Elsevier; 2021:chap 113. Kobashi KC, Vasavada S, Bloschichak A, et al. Updates to surgical treatment of female stress urinary incontinence (SUI): AUA/SUFU Guideline (2023). J Urol. 2023;209(6):1091-1098 PMID: 37096580 pubmed.ncbi.nlm.nih.gov/37096580/. Lucioni A, Kobashi KC. Evaluation and management of women with urinary incontinence and pelvic prolapse. In: Partin AW, Dmochowski RR, Kavoussi LR, Peters CA, eds. Campbell-Walsh-Wein Urology. 12th ed. Philadelphia, PA: Elsevier; 2021:chap 112. Patton S, Bassaly RM. Urinary incontinence. In: Kellerman RD, Rakel DP, Heidelbaugh JJ, Lee EM, eds. Conn's Current Therapy 2024. Philadelphia, PA: Elsevier; 2024:1201-1203. Resnick NM, DuBeau CE. Urinary incontinence. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 115. | ||
| ||
Review Date: 3/31/2024 Reviewed By: Sovrin M. Shah, MD, Associate Professor, Department of Urology, The Icahn School of Medicine at Mount Sinai, New York, NY. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


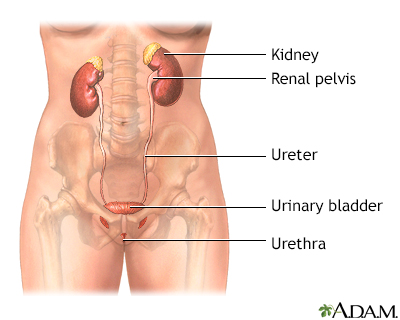 Female urinary tra...
Female urinary tra... Male urinary tract
Male urinary tract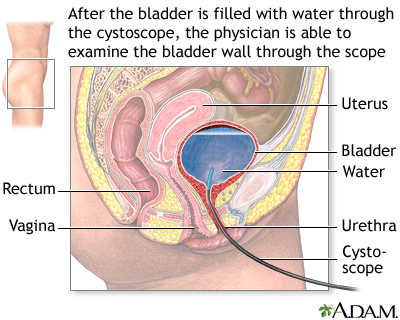 Cystoscopy
Cystoscopy