Otitis media - acute; Infection - inner ear; Middle ear infection - acute DefinitionSuspected ear infections are one of the most common reasons parents take their children to their health care provider. The most common type of ear infection is called otitis media. It is caused by swelling and infection of the middle ear. The middle ear is located just behind the eardrum. An acute ear infection starts over a short period and is painful. Ear infections that last a long time or come and go are called chronic ear infections. CausesThe eustachian tube runs from the middle of each ear to the back of the throat. Normally, this tube drains fluid that is made in the middle ear. If this tube gets blocked, fluid can build up. This can lead to infection.
Anything that causes the eustachian tubes to become swollen or blocked may lead to more fluid buildup in the middle ear behind the eardrum. Some causes are:
Ear infections are also more likely in children who spend a lot of time drinking from a sippy cup or bottle while lying on their back. Milk may enter the eustachian tube, which may increase the risk of an ear infection. Getting water in the ears will not cause an acute ear infection unless the eardrum has a hole in it. Other risk factors for acute ear infections include:
SymptomsIn infants, often the main sign of an ear infection is acting irritable or crying that cannot be soothed. Many infants and children with an acute ear infection have a fever or trouble sleeping. Tugging on the ear is not always a sign that the child has an ear infection. Symptoms of an acute ear infection in older children or adults include:
The ear infection may start shortly after a cold. Sudden drainage of yellow or green fluid from the ear may mean the eardrum has ruptured. All acute ear infections involve fluid behind the eardrum. At home, you can use an electronic ear monitor to check for this fluid. You can buy this device at a drugstore. You still need to see your child's provider to confirm an ear infection. Exams and TestsYour provider will take your medical history and ask about symptoms. Your provider will look inside the ears using an instrument called an otoscope. This exam may show:
Your provider might recommend a hearing test if you or your child has a history of ear infections. TreatmentSome ear infections clear on their own without antibiotics. Treating the pain and allowing the body time to heal itself is often all that is needed:
All children younger than 6 months with a fever or symptoms of an ear infection should see their provider. Children who are older than 6 months may be watched at home if they do not have:
If there is no improvement or if symptoms get worse, schedule an appointment with your provider to determine whether antibiotics are needed. ANTIBIOTICS A virus or bacteria can cause ear infections. Antibiotics will not help an infection that is caused by a virus. Most providers don't prescribe antibiotics for every ear infection. However, all children younger than 6 months with an ear infection are treated with antibiotics. Your provider is more likely to prescribe antibiotics if your child:
If antibiotics are prescribed, it is important to take them as directed and to take all of the medicines. Do not stop the medicine when symptoms go away. If the antibiotics do not seem to be working within 48 to 72 hours, contact your provider. You may need to switch to a different antibiotic. Side effects of antibiotics may include nausea, vomiting, and diarrhea. Serious allergic reactions are rare, but may also occur. Some children have repeat ear infections that seem to go away between episodes. They may receive a smaller, daily dose of antibiotics to prevent new infections. SURGERY If an infection does not go away with the usual medical treatment, or if a child has many ear infections over a short period of time, their provider may recommend ear tubes:
In this procedure, a tiny tube is inserted into the eardrum, keeping open a small hole that allows air to get in so fluids can drain more easily (myringotomy). The tubes often eventually fall out by themselves. Those that don't fall out may be removed in your provider's office. If the adenoids are enlarged, removing them with surgery may be considered if ear infections continue to occur. Removing tonsils does not seem to help prevent ear infections. Outlook (Prognosis)Most often, an ear infection is a minor problem that gets better. Ear infections can be treated, but they may occur again in the future. Most children will have slight short-term hearing loss during and right after an ear infection. This is due to fluid in the ear. Fluid can stay behind the eardrum for weeks or even months after the infection has cleared. Speech or language delay is uncommon. It may occur in a child who has lasting hearing loss from many repeated ear infections. Possible ComplicationsIn rare cases, a more serious infection may develop, such as:
When to Contact a Medical ProfessionalContact your provider if:
Let your provider know right away if a child younger than 6 months has a fever, even if the child doesn't have other symptoms. PreventionYou can reduce your child's risk of ear infections with the following measures:
ReferencesHaddad J. General considerations and evaluation of the ear. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 676. Pelton SI. Otitis externa, otitis media, and mastoiditis. In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. 9th ed. Philadelphia, PA: Elsevier; 2020:chap 61. Player B. Otitis media. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 680. Rosenfeld RM, Tunkel DE, Schwartz SR, et al. Clinical Practice Guideline: Tympanostomy tubes in children (update).Otolaryngol Head Neck Surg. 2022;166(1_suppl):S1-S55. PMID: 35138954 pubmed.ncbi.nlm.nih.gov/35138954/. Schilder AGM, Rosenfeld RM, Venekamp RP. Acute otitis media and otitis media with effusion. In: Flint PW, Francis HW, Haughey BH, et al, eds. Cummings Otolaryngology: Head and Neck Surgery. 7th ed. Philadelphia, PA: Elsevier; 2021:chap 199. | ||
| ||
Review Date: 1/1/2025 Reviewed By: Charles I. Schwartz, MD, FAAP, Clinical Assistant Professor of Pediatrics, Perelman School of Medicine at the University of Pennsylvania, General Pediatrician at PennCare for Kids, Phoenixville, PA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


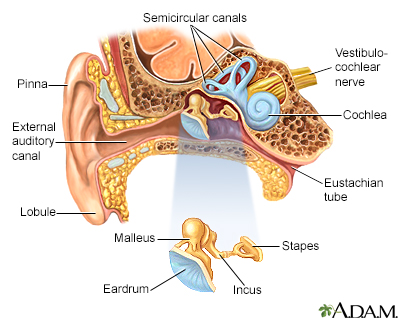 Ear anatomy
Ear anatomy Middle ear infecti...
Middle ear infecti...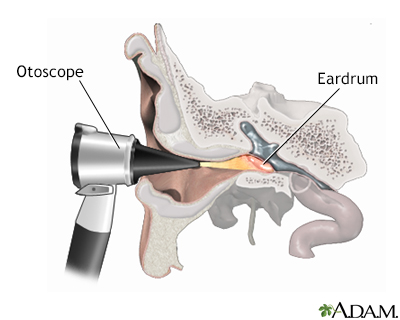 Otoscopic exam of ...
Otoscopic exam of ...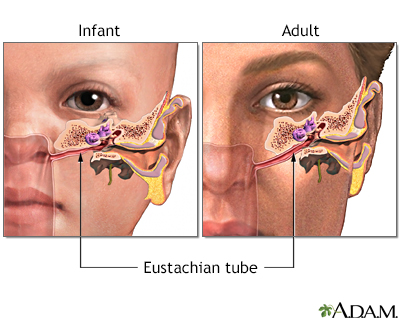 Eustachian tube
Eustachian tube Mastoiditis - side...
Mastoiditis - side...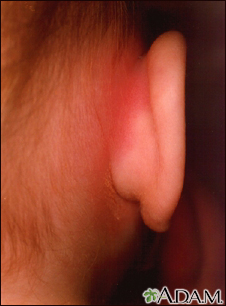 Mastoiditis - redn...
Mastoiditis - redn...