Middle ear infection - chronic; Otitis media - chronic; Chronic otitis media; Chronic ear infection DefinitionChronic ear infection is fluid, swelling, or an infection behind the eardrum that does not go away or keeps coming back. It may cause long-term or permanent damage to the ear and involves a hole in the eardrum (perforation) that does not heal. CausesThe eustachian tube runs from the middle of each ear to the back of the throat. This tube drains fluid made in the middle ear. If the eustachian tube becomes blocked, fluid can build up. When this happens, infection can occur. A chronic ear infection develops when fluid or an infection behind the eardrum does not go away. A chronic ear infection may be caused by:
Suppurative chronic otitis is a term used to describe an eardrum that keeps rupturing, draining, or swelling in the middle ear or mastoid area (the bone behind the ear) and does not go away. Ear infections are more common in children because their eustachian tubes are shorter, narrower, and more horizontal than in adults. Chronic ear infections are much less common than acute ear infections. SymptomsSymptoms of a chronic ear infection may be less severe than symptoms of an acute infection. The problem may go unnoticed and untreated for a long time. Symptoms may include:
Symptoms may continue or come and go. They may occur in one or both ears. Exams and TestsYour health care provider will look in the ears using an otoscope. The exam may reveal:
Tests may include:
TreatmentYour provider may prescribe antibiotics if the infection is caused by bacteria. These medicines may need to be taken for a long time. They may be given by mouth or into a vein (intravenously). If there is a hole in the eardrum, antibiotic ear drops are used. The provider may recommend using a mild acidic solution (such as vinegar and water) for a hard-to-treat infected ear that has a hole. A surgeon may need to clean out (debride) tissue that has gathered inside the ear. Other surgeries that may be needed include:
Outlook (Prognosis)Chronic ear infections often respond to treatment. However, your child may need to keep taking medicines for several months. Chronic ear infections are not life threatening. However, they can be uncomfortable and may result in hearing loss and other serious complications. Possible ComplicationsA chronic ear infection may cause permanent changes to the ear and nearby bones, including:
Hearing loss from damage to the middle ear may slow language and speech development. This is more likely if both ears are affected. Permanent hearing loss is rare, but the risk increases with the number and length of infections. When to Contact a Medical ProfessionalContact your provider if:
PreventionGetting prompt treatment for an acute ear infection may reduce the risk of developing a chronic ear infection. Have a follow-up exam with your provider after an ear infection has been treated to make sure that it is completely cured. ReferencesChole RA, Sharon JD. Chronic otitis media, mastoiditis, and petrositis. In: Flint PW, Francis HW, Haughey BH, et al, eds. Cummings Otolaryngology: Head and Neck Surgery. 7th ed. Philadelphia, PA: Elsevier; 2021:chap 140. Pelton SI. Otitis externa, otitis media, and mastoiditis. In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. 9th ed. Philadelphia, PA: Elsevier; 2020:chap 61. Player B. Otitis media. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 680. Rosenfeld RM, Tunkel DE, Schwartz SR, et al. Clinical Practice Guideline: Tympanostomy tubes in children (update). Otolaryngol Head Neck Surg. 2022;166(1_suppl):S1-S55. PMID: 35138954 pubmed.ncbi.nlm.nih.gov/35138954/. | ||
| ||
Review Date: 1/1/2025 Reviewed By: Charles I. Schwartz, MD, FAAP, Clinical Assistant Professor of Pediatrics, Perelman School of Medicine at the University of Pennsylvania, General Pediatrician at PennCare for Kids, Phoenixville, PA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


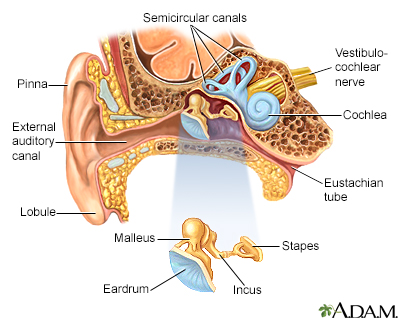 Ear anatomy
Ear anatomy Middle ear infecti...
Middle ear infecti...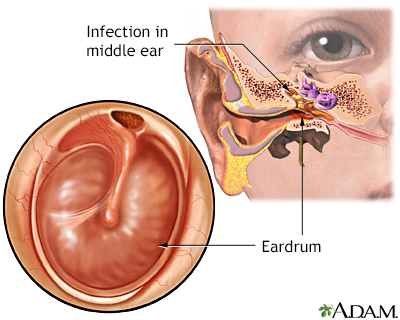 Middle ear infecti...
Middle ear infecti...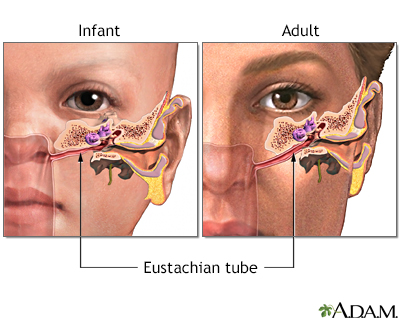 Eustachian tube
Eustachian tube