Xerostomia - Sjögren syndrome; Keratoconjunctivitis sicca - Sjögren; Sicca syndrome; Sjögren syndrome; Sjögren's syndrome DefinitionSjögren syndrome is an autoimmune disorder in which the glands that produce tears and saliva are destroyed. This causes dry mouth and dry eyes. The condition may affect other parts of the body, including the kidneys and lungs. CausesThe cause of Sjögren syndrome is unknown. It is an autoimmune disorder. This means the body attacks healthy tissue by mistake. The syndrome occurs most often in women ages 40 to 50. It is rare in children. Primary Sjögren syndrome is defined as dry eyes and dry mouth without another autoimmune disorder. Secondary Sjögren syndrome occurs along with another autoimmune disorder, such as:
SymptomsDry eyes and dry mouth are the most common symptoms of this syndrome. Eye symptoms:
Mouth and throat symptoms:
Other symptoms may include:
Exams and TestsA complete physical exam will be done. The exam reveals dry eyes and dry mouth. There may be mouth sores, decayed teeth or gum inflammation. This occurs because of the mouth dryness. Your health care provider will look in your mouth for fungus infection (candida). Skin may show a rash, the lung exam may be abnormal, the abdomen will be palpated for liver enlargement. The joints will be examined for arthritis. The neurologic exam will look for deficits due to nerve damage. You may have the following tests done:
TreatmentThe goal is to relieve symptoms.
Oral medicines such as pilocarpine or cevimeline that cause increased saliva production can be useful in dryness when local therapy is not helping. Disease-modifying antirheumatic drugs (DMARDs) similar to those used for RA may improve the symptoms of Sjögren syndrome. These include Rituximab and tumor necrosis factor (TNF) inhibiting drugs such as etanercept (Enbrel), adalimumab (Humira) or infliximab (Remicade). Some things you can do to ease symptoms include:
Talk with your dentist about:
To prevent dental decay caused by mouth dryness:
Outlook (Prognosis)The disease is most often not life threatening. The outcome depends on what other diseases you have. There is a higher risk for lymphoma and early death when Sjögren syndrome has been very active for a long time, as well as in people with vasculitis, low complements, and cryoglobulins. Possible ComplicationsComplications may include:
When to Contact a Medical ProfessionalContact your provider if you develop symptoms of Sjögren syndrome. ReferencesPang R, Ma X, Guo H, Qi X. Meta-analysis of mortality-associated factors in primary Sjögren's syndrome patients with interstitial lung disease. Clin Rheumatol. 2025;44(1):23-31. PMID: 39432139 pubmed.ncbi.nlm.nih.gov/39432139/. St. Clair EW. Sjögren syndrome. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 247. St. Clair EW, Leverenz DL. Sjögren syndrome. In: Firestein GS, McInnes IB, Koretzky GA, Mikuls TR, Neogi T, O'Dell JR, eds. Firestein & Kelley's Textbook of Rheumatology. 12th ed. Philadelphia, PA: Elsevier; 2025:chap 74. Turner MD. Oral manifestations of systemic diseases. In: Flint PW, Francis HW, Haughey BH, et al, eds. Cummings Otolaryngology: Head and Neck Surgery. 7th ed. Philadelphia, PA: Elsevier; 2021:chap 12. | ||
| ||
Review Date: 4/1/2025 Reviewed By: Diane M. Horowitz, MD, Rheumatology and Internal Medicine, Northwell Health, Great Neck, NY. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


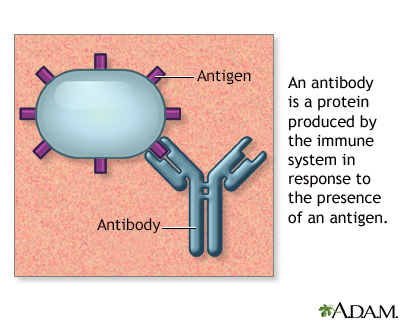 Antibodies
Antibodies