Lumbar radiculopathy; Cervical radiculopathy; Herniated intervertebral disk; Prolapsed intervertebral disk; Slipped disk; Ruptured disk; Herniated nucleus pulposus; Low back pain - herniated disk; LBP - herniated disk; Sciatica - herniated disk; Herniated disk; Disc - herniated DefinitionA herniated (slipped) disk occurs when all or part of a disk is forced through a weakened part of the disk. This may place pressure on nearby nerves or the spinal cord. CausesThe bones (vertebrae) of the spinal column protect nerves that come out of the brain and travel down your back to form the spinal cord. Nerve roots are large nerves that branch out from the spinal cord and leave your spinal column between each vertebra. The spinal bones are separated by disks. These disks cushion the spinal column and put space between your vertebrae. The disks allow movement between the vertebrae, which lets you bend and reach. With herniated disk:
A herniated disk is a cause of radiculopathy. This is a condition that affects one or more of the spinal nerve roots. Herniated disks occur more often in middle-aged and older men, usually after strenuous activity. Other risk factors may include:
SymptomsThe pain most often occurs on one side of the body. Symptoms vary, depending on the site of injury, and may include the following:
The pain often starts slowly. It may get worse:
You may also have weakness in certain muscles. Sometimes, you may not notice it until your health care provider examines you. In other cases, you will notice that you have a hard time lifting your leg or arm, standing on your toes on one side, squeezing tightly with one of your hands, or other problems. You may lose control of your bladder or bowels. The pain, numbness, or weakness often goes away or improves a lot over weeks to months. Exams and TestsA careful physical exam and history is the first step. Depending on where you have symptoms, your provider examines your neck, shoulder, arms, and hands, or your lower back, hips, legs, and feet. Your provider will check:
Your provider may also ask you to:
Leg pain that occurs when you sit on an exam table and lift your leg straight up usually suggests a herniated disk in your lower back. In another test, you will bend your head forward and to the sides while the provider puts slight downward pressure on the top of your head. Increased pain or numbness during this test is usually a sign of pressure on a nerve in your neck. DIAGNOSTIC TESTS Tests that may be done may include:
TreatmentThe first treatment for a slipped disk is a short period of rest and taking medicines for the pain. This is usually followed by physical therapy. Most people who follow these treatments recover and return to normal activities. Some people will need to have more treatment. This may include steroid injections or surgery. MEDICINES Medicines can help with your pain. Your provider may prescribe any of the following:
LIFESTYLE CHANGES If you are overweight, diet and exercise are very important for improving back pain. Physical therapy is important for nearly everyone with disk disease. Therapists will teach you how to properly lift, dress, walk, and perform other activities. They will teach you how to strengthen muscles that help support the spine. You will also learn how to increase flexibility in your spine and legs. Take care of your back at home:
INJECTIONS Steroid medicine injections into the back in the area of the herniated disk may help control pain for several months. These injections reduce swelling around the spinal nerve and disk and relieve many symptoms. They do not solve the underlying problem and your pain may return after weeks or months. Spinal injections are an outpatient procedure. SURGERY Surgery may be an option if your symptoms do not go away with other treatments and time. One such surgery is diskectomy, which removes all or part of a disk. Discuss with your provider which treatment options are best for you. Outlook (Prognosis)Most people improve with treatment. But you may have long-term back pain, even after treatment. It may take several months to a year or more to go back to all of your activities without having pain or straining your back. People who work in jobs that involve heavy lifting or back strain may need to change their job activities to avoid injuring their back again. Possible ComplicationsIn rare cases, the following problems can occur:
When to Contact a Medical ProfessionalContact your provider if you have:
PreventionTo help prevent back injury:
Your provider may suggest a back brace to help support the spine. A brace may prevent injuries in people who lift heavy objects at work. But using these devices too much can weaken the muscles that support your spine and make the problem worse. ReferencesFarrell SE, Ma ZB. Musculoskeletal back pain. In: Walls RM, eds. Rosen's Emergency Medicine: Concepts and Clinical Practice. 10th ed. Philadelphia, PA: Elsevier; 2023:chap 104. Gardocki RJ, Park AL. Degenerative disorders of the thoracic and lumbar spine. In: Azar FM, Beaty JH, eds. Campbell's Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021:chap 39. Magee DJ, Manske RC. Lumbar spine. In: Magee DJ, Manske RC, eds. Orthopedic Physical Assessment. 7th ed. St Louis, MO: Elsevier; 2021:chap 9. | ||
| ||
Review Date: 8/27/2024 Reviewed By: C. Benjamin Ma, MD, Professor, Chief, Sports Medicine and Shoulder Service, UCSF Department of Orthopaedic Surgery, San Francisco, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


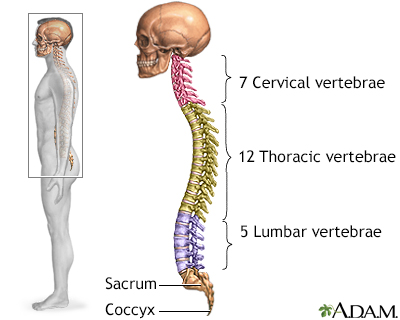 Skeletal spine
Skeletal spine Sciatic nerve
Sciatic nerve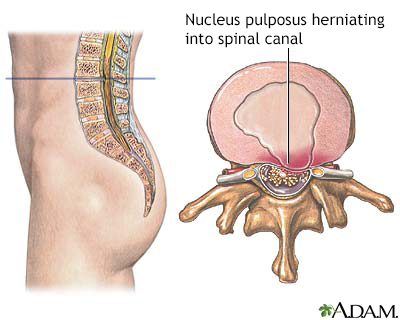 Herniated nucleus ...
Herniated nucleus ...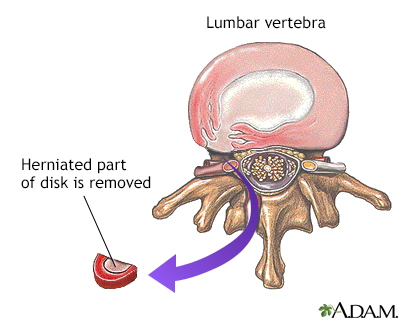 Herniated disk rep...
Herniated disk rep...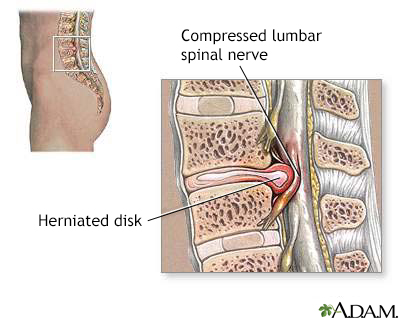 Herniated lumbar d...
Herniated lumbar d...