Pseudo-claudication; Central spinal stenosis; Foraminal spinal stenosis; Degenerative spine disease; Back pain - spinal stenosis; Low back pain - stenosis; LBP - stenosis DefinitionSpinal stenosis is narrowing of the spinal column that causes pressure on the spinal cord, or narrowing of the openings (called neural foramina) where spinal nerves leave the spinal column. CausesSpinal stenosis usually occurs as a person ages, however, some people are born with less space for their spinal cord.
Spinal stenosis may also be caused by:
SymptomsSymptoms often get worse slowly over time. Most often, symptoms will be on one side of the body, but may involve both legs. Symptoms include:
Symptoms are more likely to be present or get worse when you stand or walk. They often lessen or disappear when you sit down or lean forward. Most people with spinal stenosis cannot walk for a long period without having significant pain. More serious symptoms include:
Exams and TestsDuring a physical exam, your health care provider will try to find the location of the pain and learn how it affects your movement. You will be asked to:
Your provider will also move your legs in different positions, including bending and straightening your knees. This is to check your strength and ability to move. To test nerve function, your provider will use a rubber hammer to check your reflexes. To test how well your nerves sense feeling, your provider will touch your legs in many places with a pin, cotton swab, or feather. To check your balance, your provider will ask you to close your eyes while standing and keeping your feet together. A brain and nervous system (neurologic) exam helps confirm leg weakness and loss of sensation in the legs. You may have the following tests: TreatmentYour provider and other health professionals will help you manage your pain and keep you as active as possible.
Treatments for back pain caused by spinal stenosis include:
Spinal stenosis symptoms often become worse over time, but this may happen slowly. If the pain does not respond to these treatments, or you lose movement or feeling, you may need surgery.
Surgery may include removing a bulging disk, removing part of the vertebra bone, or widening the canal and openings where your spinal nerves are located. During some spinal surgeries, the surgeon will remove some bone to create more room for your spinal nerves or spinal column. The surgeon will then fuse some of the spine bones to make your spine more stable. But this will make your back more stiff and may cause arthritis in areas above or below your fused spine. Outlook (Prognosis)Many people with spinal stenosis are able to be active with the condition, although they may need to make some changes in their activities or work. Spine surgery will often partly or fully relieve symptoms in your legs or arms. It is hard to predict if you will improve and how much relief surgery will provide.
In rare cases, injuries caused by pressure on the nerves are permanent, even if the pressure is relieved. When to Contact a Medical ProfessionalContact your provider if you have symptoms of spinal stenosis. More serious symptoms that need prompt attention include:
ReferencesBussières A, Cancelliere C, Ammendolia C, et al. Non-surgical interventions for lumbar spinal stenosis leading to neurogenic claudication: a clinical practice guideline. J Pain. 2021;22(9):1015-1039 PMID: 3385761 pubmed.ncbi.nlm.nih.gov/33857615/. Gardocki RJ, Park AL. Degenerative disorders of the thoracic and lumbar spine. In: Azar FM, Beaty JH, eds. Campbell's Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021:chap 39. Issac Z, Sarno D. Lumbar spinal stenosis. In: Frontera WR, Silver JK, Rizzo TD Jr, eds. Essentials of Physical Medicine and Rehabilitation. 4th ed. Philadelphia, PA: Elsevier; 2019:chap 50. Katz JN, Zimmerman ZE, Mass H, Makhni MC. Diagnosis and management of lumbar spinal stenosis: a review. JAMA. 2022;327(17):1688-1699 PMID: 35503342 pubmed.ncbi.nlm.nih.gov/35503342/. | ||
| ||
Review Date: 8/27/2024 Reviewed By: C. Benjamin Ma, MD, Professor, Chief, Sports Medicine and Shoulder Service, UCSF Department of Orthopaedic Surgery, San Francisco, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


 Sciatic nerve
Sciatic nerve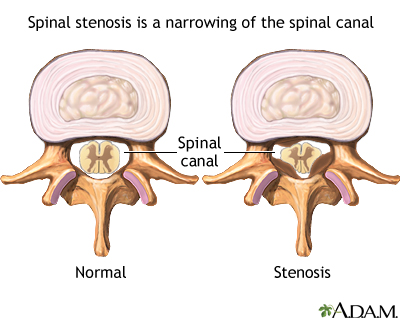 Spinal stenosis
Spinal stenosis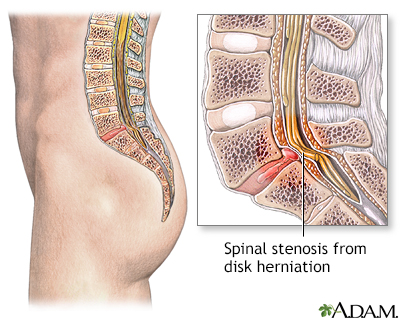 Spinal stenosis
Spinal stenosis