Plaque psoriasis; Psoriasis vulgaris; Guttate psoriasis; Pustular psoriasis DefinitionPsoriasis is a skin condition that causes skin redness, silvery scales, and irritation. Most people with psoriasis have thick, red, well-defined patches of skin with flaky, silver-white scales. This is called plaque psoriasis. CausesPsoriasis is common. Anyone can develop it, but it most often begins between ages 10 and 35, or as people get older. Psoriasis isn't contagious. This means it doesn't spread to other people. Psoriasis seems to be inherited through families, at least to some degree. Normal skin cells grow deep in the skin and rise to the surface about once a month. When you have psoriasis, on average this process takes place within 7 to14 days. This results in dead skin cells building up on the skin's surface, forming the collections of scales. The following may trigger an attack of psoriasis or make it harder to treat:
Psoriasis may be worse in people who have a weak immune system, including people with HIV/AIDS. Some people with psoriasis also have arthritis (psoriatic arthritis). People with psoriasis have an increased risk for fatty liver disease and cardiovascular disorders, such as heart disease and stroke. SymptomsPsoriasis can appear suddenly or slowly. Many times, it goes away and then comes back. The main symptom of the condition is irritated, red, flaky plaques of skin. Plaques are most often seen on the elbows, knees, and middle of the body. But they can appear anywhere, including on the scalp, palms, soles of the feet, and genitals. The skin may be:
Other symptoms may include:
There are five main types of psoriasis:
Exams and TestsYour health care provider can usually diagnose this condition by looking at your skin. Sometimes, a skin biopsy is done to check for other possible conditions. If you have joint pain, your provider may order imaging studies. TreatmentThe goal of treatment is to regulate your symptoms and prevent infection. Three treatment options are available:
TREATMENTS USED ON THE SKIN (TOPICAL) Most of the time, psoriasis is treated with medicines that are placed directly on the skin or scalp. These may include:
SYSTEMIC (BODY-WIDE) TREATMENTS If you have moderate to severe psoriasis, your provider will likely recommend medicines that suppress the immune system's faulty response. These medicines include methotrexate or cyclosporine. Retinoids such as acitretin can also be used. Newer medicines, called biologics, are more commonly used as they more specifically target the causes of psoriasis. Biologics approved for the treatment of psoriasis include:
PHOTOTHERAPY Some people may choose to have phototherapy, which is safe and can be very effective:
OTHER TREATMENTS If you have an infection, your provider will prescribe antibiotics. HOME CARE Following these tips at home may help:
Support GroupsSome people may benefit from a psoriasis support group. The National Psoriasis Foundation is a good resource: www.psoriasis.org. Outlook (Prognosis)Psoriasis can be a lifelong condition that usually can be controlled with treatment. It may go away for a long time and then return. With proper treatment, it will not affect your overall health. But be aware that there is a strong link between psoriasis and other health problems, such as heart disease. When to Contact a Medical ProfessionalContact your provider if you have symptoms of psoriasis or if your skin irritation continues despite treatment. Tell your provider if you have joint pain or fever with your psoriasis attacks. If you have symptoms of arthritis, talk to your provider, dermatologist or rheumatologist. Go to the emergency room or call 911 or the local emergency number if you have a severe outbreak that covers all or most of your body. PreventionThere is no known way to prevent psoriasis. Keeping the skin clean and moist and avoiding your psoriasis triggers may help reduce the number of flare-ups. Providers recommend daily baths or showers for people with psoriasis. Avoid scrubbing too hard, because this can irritate the skin and trigger an attack. ReferencesArmstrong AW, Siegel MP, Bagel J, et al. From the Medical Board of the National Psoriasis Foundation: treatment targets for plaque psoriasis. J Am Acad Dermatol. 2017;76(2):290-298. PMID: 27908543 pubmed.ncbi.nlm.nih.gov/27908543/. Dinulos JGH. Psoriasis and other papulosquamous diseases. In: Dinulos JGH, ed. Habif's Clinical Dermatology. 7th ed. Philadelphia, PA: Elsevier; 2021:chap 8. Lebwohl MG, van de Kerkhof P. Psoriasis. In: Lebwohl MG, Heymann WR, Coulson IH, Murrell DF, eds. Treatment of Skin Disease. 6th ed. Philadelphia, PA: Elsevier; 2022:chap 210. van de Kerkhof PCM, Iversen L. Psoriasis. In: Bolognia JL, Schaffer JV, Cerroni L, eds. Dermatology. 5th ed. Philadelphia, PA: Elsevier; 2025:chap 8. | ||
| ||
Review Date: 8/5/2024 Reviewed By: Elika Hoss, MD, Assistant Professor of Dermatology, Mayo Clinic, Scottsdale, AZ. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


 Psoriasis on the k...
Psoriasis on the k...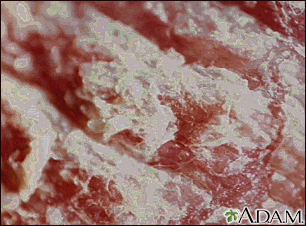 Psoriasis - magnif...
Psoriasis - magnif... Psoriasis - guttat...
Psoriasis - guttat...