Hypertrophic osteoarthritis; Osteoarthrosis; Degenerative joint disease; DJD; OA; Arthritis - osteoarthritis DefinitionOsteoarthritis (OA) is the most common joint disorder. It is due to aging and wear and tear on a joint. CausesCartilage is the firm, rubbery tissue that cushions your bones at the joints. It allows bones to glide over one another when the joint moves. When the cartilage breaks down and wears away, the fragments of the cartilage or the bones rub together. This often causes the pain, swelling, and stiffness of OA. As OA worsens, bony spurs or extra bone may form around the joint. The ligaments and muscles around the joint may become weaker and stiffer. Before age 55, OA occurs equally in men and women. After age 55, it is more common in women. Other factors can also lead to OA.
Medical conditions that can lead to OA or symptoms similar to OA include:
SymptomsSymptoms of OA often appear in middle age. Almost everyone has some symptoms of OA by age 70. Pain and stiffness in the joints are the most common symptoms. The pain is often worse:
With OA, your joints may become stiffer and harder to move over time. You may notice a rubbing, grating, or crackling sound when you move the joint. Morning stiffness refers to the pain and stiffness you feel when you first wake up in the morning. Stiffness due to OA often lasts for 30 minutes or less. It can last more than 30 minutes if there is inflammation in the joint. It often improves after activity, allowing the joint to warm up. During the day, the pain may get worse when you are active and feel better when you are resting. As OA gets worse, you may have pain even when you are resting. And it may wake you up at night. Some people might not have symptoms, even though x-rays show the physical changes of OA. Exams and TestsYour health care provider will examine you and ask about your symptoms. The exam may show:
Blood tests are not helpful in diagnosing OA. They can be used to look for alternative conditions, such as rheumatoid arthritis or gout. An x-ray will likely show:
TreatmentOA cannot be cured, but OA symptoms can be controlled. OA will most likely get worse over time though the pace with which this occurs varies from person to person. You can have surgery, but other treatments can improve your pain and make your life much better. Although these treatments cannot make the OA go away, they can often delay surgery or make your symptoms mild enough to not cause significant problems. MEDICINES Over-the-counter (OTC) pain relievers, such as acetaminophen (Tylenol) or a nonsteroidal anti-inflammatory drug (NSAID) can help with OA symptoms. You can buy these medicines without a prescription. It is recommended that you should not take more than 3 grams (3,000 milligrams) of acetaminophen a day. If you have liver disease, talk with your provider before taking acetaminophen. Over the counter NSAIDs include aspirin, ibuprofen, and naproxen. Several other NSAIDs are available by prescription. Talk with your provider before taking an NSAID on a regular basis. Duloxetine (Cymbalta) is a prescription medicine that can also help treat long-term (chronic) pain related to OA. Injections of steroid medicines into the arthritic joint often provide significant short to medium-term benefits from the pain of OA. Other medicines that may help include:
LIFESTYLE CHANGES Staying active and getting exercise can maintain joint and overall movement. Ask your provider to recommend an exercise routine or refer you to a physical therapist. Water exercises, such as swimming, are often helpful. Other lifestyle tips include:
If the pain from OA gets worse, keeping up with activities may become more difficult or painful. Making changes around the home can help take stress off your joints to relieve some of the pain. If your work is causing stress in certain joints, you may need to adjust your work area or change work tasks. PHYSICAL THERAPY Physical therapy can help improve muscle strength and the motion of stiff joints as well as your balance. If therapy does not make you feel better after 6 to 12 weeks, then it likely will not be helpful. Massage therapy may provide short-term pain relief but does not change the underlying OA process. Make sure you work with a licensed massage therapist who is experienced in working on sensitive joints. BRACES Splints and braces may help support weakened joints. Some types limit or prevent the joint from moving. Others may shift pressure off one portion of a joint. Use a brace only when your provider or therapist recommends one. Using a brace the wrong way can cause joint damage, stiffness, and pain. ALTERNATIVE TREATMENTS Acupuncture is a traditional Chinese treatment. It is thought that when acupuncture needles stimulate certain points on the body, chemicals that block pain are released. Acupuncture may provide significant pain relief for OA. Yoga and Tai chi have also shown significant benefit in treating the pain from OA. S-adenosylmethionine (SAMe, pronounced Sammy) is a manmade form of a natural chemical in the body. It may help reduce joint inflammation and pain. SURGERY Severe cases of OA might benefit from surgery to replace or repair damaged joints. Options include:
Support GroupsOrganizations that specialize in arthritis are good resources for more information on OA. Outlook (Prognosis)Your movement may become limited over time. Doing everyday activities, such as personal hygiene, household chores, or cooking may become a challenge. Treatment usually improves function. When to Contact a Medical ProfessionalContact your provider if you have symptoms of OA that are bothersome or get worse. PreventionTry not to overuse a painful joint at work or during activities. Maintain a normal body weight. Keep the muscles around your joints strong, especially the weight-bearing joints (knee, hip, or ankle). ReferencesHunter DJ. Osteoarthritis. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 241. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken). 2020;72(2):149-162. PMID: 31908149 pubmed.ncbi.nlm.nih.gov/31908149/. Misra D, Kumar D, Neogi T. Treatment of osteoarthritis. In: Firestein GS, Budd RC, Gabriel SE, Koretzky GA, McInnes IB, O'Dell JR, eds. Firestein & Kelley's Textbook of Rheumatology. 11th ed. Philadelphia, PA: Elsevier; 2021:chap 106. | ||
| ||
Review Date: 5/20/2024 Reviewed By: Jacob Berman, MD, MPH, Clinical Assistant Professor of Medicine, Division of General Internal Medicine, University of Washington School of Medicine, Seattle, WA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


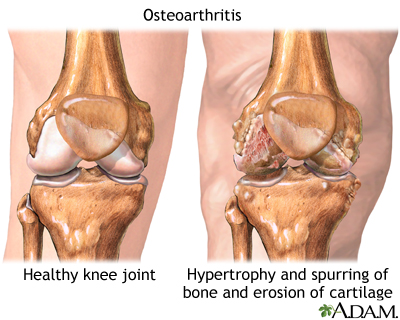 Osteoarthritis
Osteoarthritis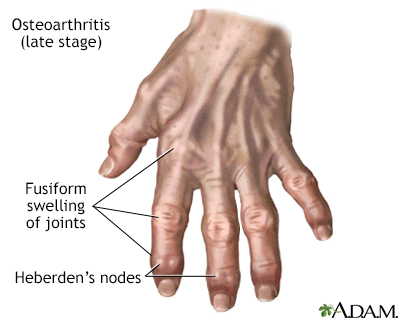 Osteoarthritis
Osteoarthritis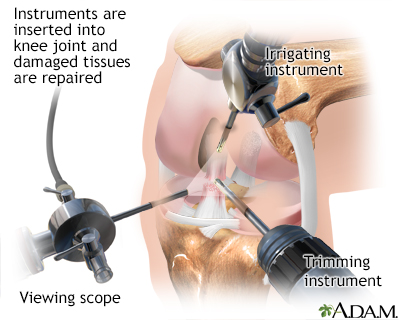 Arthroscopy
Arthroscopy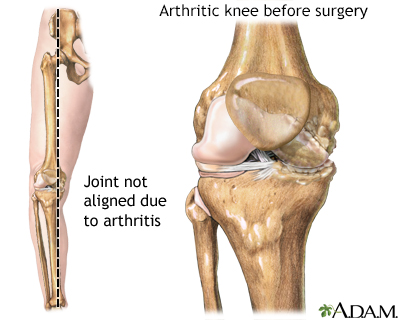 Knee misaligned du...
Knee misaligned du...