Calcium pyrophosphate dihydrate deposition disease; CPPD disease; Acute/chronic CPPD arthritis; Pseudogout; Pyrophosphate arthropathy; Chondrocalcinosis DefinitionCalcium pyrophosphate dihydrate (CPPD) arthritis is a joint disease that can cause attacks of arthritis. Like gout, crystals form in the joints. But in this arthritis, the crystals are not formed from uric acid. CausesDeposition of calcium pyrophosphate dihydrate (CPPD) causes this form of arthritis. The buildup of this chemical forms crystals in the cartilage of joints. This leads to attacks of joint swelling and pain most often in the knees, wrists, ankles, and shoulders. Other joints can be affected as well. In contrast to gout, the metatarsal-phalangeal joint of the big toe is not affected. Among older adults, CPPD is a common cause of sudden (acute) arthritis in one joint. The attack may be caused by:
CPPD arthritis mainly affects the elderly because joint degeneration and osteoarthritis increases with age. Such joint damage increases the tendency of CPPD deposition. However, CPPD arthritis is also more common in people with:
SymptomsIn most cases, CPPD deposits do not cause any symptoms. Instead, x-rays of affected joints such as knees show characteristic deposits of calcium. Some people with chronic CPPD deposits in large joints may have the following symptoms:
Attacks of joint pain can last for months. There may be no symptoms between attacks. In some people CPPD arthritis causes severe damage to a joint. CPPD arthritis can also occur in the upper and lower spine. Pressure on spinal nerves may cause pain in the arms or legs. Because the symptoms are similar, CPPD arthritis can be confused with:
Exams and TestsMost arthritic conditions show similar symptoms. Carefully testing the joint fluid for crystals can help the health care provider diagnose the condition. You may undergo the following tests:
TreatmentTreatment may involve removing fluid to relieve pressure in the joint. A needle is placed into the joint and fluid is aspirated. Some common treatment options are:
Outlook (Prognosis)Most people do well with treatment to reduce the acute joint pain. A medicine such as colchicine may help prevent repeat attacks. There is no treatment to remove the CPPD crystals. Possible ComplicationsPermanent joint damage can occur without treatment. When to Contact a Medical ProfessionalContact your provider if you have attacks of joint swelling and joint pain. PreventionThere is no known way to prevent this disorder. However, treating other problems that may cause CPPD arthritis may make the condition less severe. Regular follow-up visits may help prevent permanent damage of the affected joints. ReferencesEdwards NL. Crystal deposition diseases. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 252. Terkeltaub R. Calcium crystal disease: calcium pyrophosphate dihydrate and basic calcium phosphate. In: Firestein GS, Budd RC, Gabriel SE, Koretzky GA, McInnes IB, O'Dell JR, eds. Firestein & Kelley's Textbook of Rheumatology. 11th ed. Philadelphia, PA: Elsevier; 2021:chap 102. | ||
| ||
Review Date: 3/31/2024 Reviewed By: Neil J. Gonter, MD, Assistant Professor of Medicine, Columbia University, NY and private practice specializing in Rheumatology at Rheumatology Associates of North Jersey, Teaneck, NJ. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


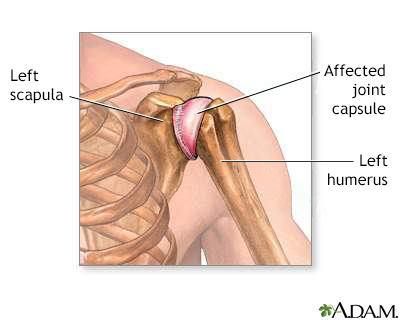 Shoulder joint inf...
Shoulder joint inf...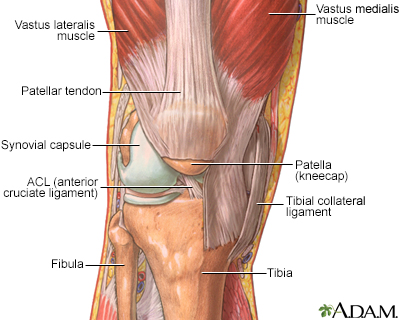 The structure of a...
The structure of a...