Adrenal tumor - Cushing syndrome; Cushing syndrome due to adrenal tumor DefinitionCushing syndrome due to adrenal tumor is a form of Cushing syndrome. It occurs when a tumor of the adrenal gland releases excess amounts of the hormone cortisol. CausesCushing syndrome is a group of symptoms and signs that occurs when your body has a higher than normal level of the hormone cortisol. This hormone is made in the adrenal glands. Too much cortisol can be due to various problems. One such problem is a tumor on one of the adrenal glands. Adrenal tumors release cortisol. Adrenal tumors are rare. They can be noncancerous (benign) or cancerous (malignant). Noncancerous tumors that can cause Cushing syndrome include:
Cancerous tumors that may cause Cushing syndrome include an adrenal carcinoma. This is a rare tumor, but it usually makes excess cortisol. SymptomsMost people with Cushing syndrome have:
Skin changes that are often seen:
Muscle and bone changes include:
Body-wide (systemic) changes include:
Women often have:
Men may have:
Other symptoms that may occur include:
Exams and TestsYour health care provider will perform a physical exam and ask about your symptoms. Tests to confirm Cushing syndrome:
Tests to determine cause or complications include:
In some cases, you need a special test called adrenal vein sampling to determine which adrenal gland is making too much cortisol and causing Cushing syndrome. TreatmentSurgery is done to remove the adrenal tumor. Often, the entire adrenal gland is removed. Glucocorticoid replacement treatment is usually needed until the other adrenal gland recovers from surgery. You may need this treatment for 3 to 12 months. If surgery is not possible, such as in cases of adrenal cancer that has spread (metastasis), medicines can be used to stop the release of cortisol. Outlook (Prognosis)People with an adrenal tumor who have surgery have an excellent outlook. For adrenal cancer, surgery is sometimes not possible. When surgery is performed, it does not always cure the cancer. Possible ComplicationsCancerous adrenal tumors can spread to the liver or lungs. When to Contact a Medical ProfessionalContact your provider if you develop any symptoms of Cushing syndrome. PreventionAppropriate treatment of adrenal tumors may reduce the risk of complications in some people with adrenal tumor-related Cushing syndrome. ReferencesAsban A, Patel AJ, Reddy S, Wang T, Balentine CJ, Chen H. Cancer of the endocrine system. In: Niederhuber JE, Armitage JO, Kastan MB, Doroshow JH, Tepper JE, eds. Abeloff's Clinical Oncology. 6th ed. Philadelphia, PA: Elsevier; 2020:chap 68. Auchus RJ, Pandey CEF. The adrenal cortex. In: Melmed S, Auchus RJ, Goldfine AB, Rosen CJ, Kopp PA, eds. Williams Textbook of Endocrinology. 15th ed. Philadelphia, PA: Elsevier; 2025:chap 13. Fragaso MCBV, Berthon A, Bertherat J. Adrenocorticotropic hormone–independent Cushing syndrome. In: Robertson RP, ed. DeGroot's Endocrinology. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 97. Nieman LK. Adrenal cortex. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 208. | ||
| ||
Review Date: 4/24/2025 Reviewed By: Sandeep K. Dhaliwal, MD, board-certified in Diabetes, Endocrinology, and Metabolism, Springfield, VA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


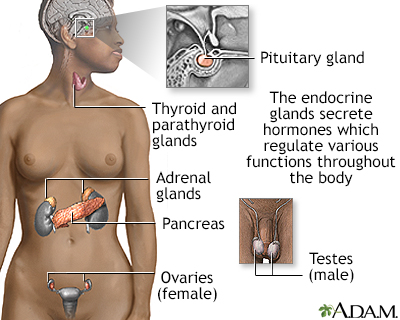 Endocrine glands
Endocrine glands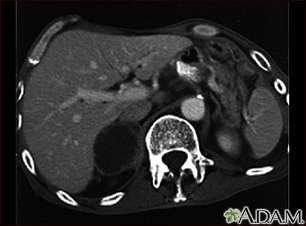 Adrenal metastases...
Adrenal metastases...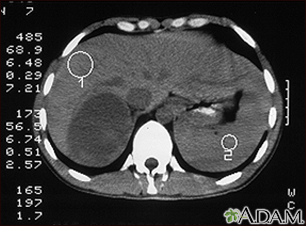 Adrenal Tumor - CT
Adrenal Tumor - CT