Adrenal crisis; Addisonian crisis; Acute adrenal insufficiency DefinitionAcute adrenal crisis is a life-threatening condition that occurs when there is not enough cortisol. This is a hormone produced by the adrenal glands. CausesThe adrenal glands are small hormone-releasing organs located on top of each kidney. They are made up of an outer portion called the cortex, and an inner portion called the medulla. The cortex produces 3 hormones:
The medulla produces the hormone adrenaline (also called epinephrine). Both cortisol and adrenaline are released in response to stress. Cortisol production is regulated by the pituitary. This is a small gland just underneath the brain. The pituitary releases adrenocorticotropic hormone (ACTH). This is a hormone that causes the adrenal glands to release cortisol. Adrenaline production is regulated by nerves coming from the brain and spinal cord and by circulating hormones. Adrenal crisis can occur from any of the following:
SymptomsSymptoms and signs of adrenal crisis can include any of the following:
Exams and TestsTests that may be ordered to help diagnose acute adrenal crisis include:
TreatmentAdrenal crisis is a medical emergency. In adrenal crisis, you need to be given the medicine hydrocortisone right away through a vein (intravenous) or muscle (intramuscular). You may receive intravenous fluids if you have low blood pressure. You will need to go to the hospital for treatment and monitoring. If infection or another medical problem caused the crisis, you may need additional treatment. Many people with primary or secondary adrenal insufficiency have an emergency syringe with hydrocortisone at home that a family member can inject into muscle if they are too sick or too weak to take their hydrocortisone pills. Outlook (Prognosis)Shock may occur if treatment is not provided early, and it can be life threatening from very low blood pressure and heart problems. When to Contact a Medical ProfessionalGo to the emergency room or call the local emergency number (such as 911) if you develop symptoms of acute adrenal crisis. Contact your health care provider if you have Addison disease or hypopituitarism and are unable to take your glucocorticoid medicine for any reason. If you have Addison disease, you will usually be told to temporarily increase the dosage of your glucocorticoid medicine if you are stressed or ill, or before having surgery. This is called stress or sick-day dosing. PreventionIf you have Addison disease, learn to recognize the signs of potential stress that may cause an acute adrenal crisis. If you have been instructed by your provider, be prepared to give yourself an emergency shot of glucocorticoid or to increase your dosage of oral glucocorticoid medicine in times of stress. Parents should learn to do this for their children who have adrenal insufficiency. Always carry medical ID (card, bracelet, or necklace) that says you have adrenal insufficiency. The ID should also say the type of medicine and dosage you need in case of an emergency. If you take glucocorticoid medicines for pituitary ACTH deficiency, be sure you know when to take a stress dose of your medicine. Discuss this with your provider. Never miss taking your medicines. ReferencesAuchus RJ, Pandey CEF. The adrenal cortex. In: Melmed S, Auchus RJ, Goldfine AB, Rosen CJ, Kopp PA, eds. Williams Textbook of Endocrinology. 15th ed. Philadelphia, PA: Elsevier; 2025:chap 13. Bornstein SR, Allolio B, Arlt W, et al. Diagnosis and treatment of primary adrenal insufficiency: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(2):364-389. PMID: 26760044 pubmed.ncbi.nlm.nih.gov/26760044/. Nieman LK. Adrenal cortex. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 208. Thiessen MEW. Thyroid and adrenal disorders. In: Walls RM, ed. Rosen's Emergency Medicine: Concepts and Clinical Practice. 10th ed. Philadelphia, PA: Elsevier; 2023:chap 117. | ||
| ||
Review Date: 4/24/2025 Reviewed By: Sandeep K. Dhaliwal, MD, board-certified in Diabetes, Endocrinology, and Metabolism, Springfield, VA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


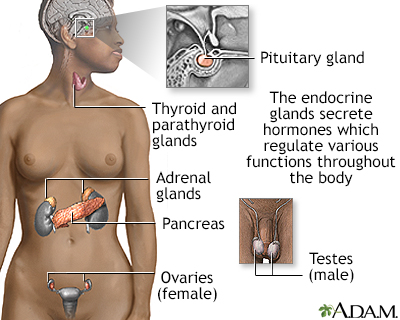 Endocrine glands
Endocrine glands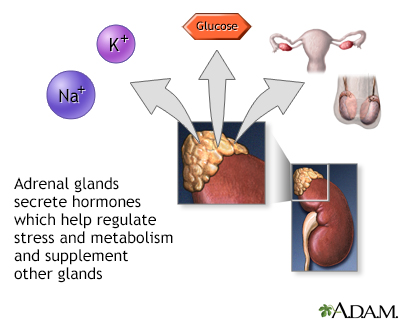 Adrenal gland horm...
Adrenal gland horm...