Adenoma - secreting; Prolactin - secreting adenoma of the pituitary DefinitionA prolactinoma is a noncancerous (benign) pituitary tumor that produces a hormone called prolactin. This results in too much prolactin in the blood. CausesProlactin is a hormone that triggers the breasts to produce milk (lactation). Prolactinoma is the most common type of pituitary tumor (adenoma) that produces a hormone. It accounts for about 50% of all pituitary adenomas. Almost all pituitary tumors are noncancerous (benign). Prolactinoma may occur as part of an inherited condition called multiple endocrine neoplasia type 1 (MEN 1). Prolactinomas occur most commonly in people in their 20s and 30s. They are more common in women than in men and are rare in children. At least half of all prolactinomas are very small (less than 3/8 of an inch or 1 centimeter [cm] in diameter). These small tumors occur more often in women and are called microprolactinomas. Tumors larger than 3/8 inch (in) or 1 centimeter (cm) in diameter are called macroprolactinomas. Larger tumors are more common in men. They tend to occur at an older age. The tumor can grow to a large size before symptoms appear. The tumor is often detected at an earlier stage in young women than in men because the high prolactin causes irregular menstrual periods. SymptomsIn women:
In men:
Symptoms caused by pressure from a larger tumor may include:
There may be no symptoms, especially in older men. Exams and TestsYour health care provider will perform a physical exam and ask about your symptoms. You will also be asked about medicines and substances you are taking. Tests that may be ordered include:
TreatmentMedicine is usually successful in treating prolactinoma. Some people have to take these medicines for life. Other people can stop taking the medicines after 2 to 3 years, especially if their tumor was small (less than 1 cm) when it was discovered or has disappeared from the MRI images. But there is a risk that the tumor may grow and produce prolactin again, especially if it was a large tumor. A large prolactinoma can sometimes get larger during pregnancy. Surgery may be done for any of the following:
Radiation is usually only used in people with a prolactinoma that continues to grow or gets worse after both medicine and surgery have been tried. Radiation may be given in the form of:
Outlook (Prognosis)The outlook is usually excellent but depends on the success of medical treatment or surgery. Getting tested to check whether the tumor has returned after treatment is important. Treatment for prolactinoma may change the levels of other hormones in the body, especially if surgery or radiation is performed. High levels of estrogen or testosterone may be involved in the growth of a prolactinoma. Women with prolactinomas should be followed closely during pregnancy. They should discuss this tumor with their provider before taking birth control pills with a higher than usual estrogen content. Untreated pituitary adenomas always have a small risk of suddenly getting bigger, most commonly from bleeding inside the tumor. This is called pituitary apoplexy, and it is a medical emergency. Most people with pituitary apoplexy describe it as having the worst headache of their life. When to Contact a Medical ProfessionalContact your provider if you have any symptoms of prolactinoma. If you have had a prolactinoma in the past, contact your provider for a general follow-up, or if your symptoms return. ReferencesCooper PE, Van Uum SHM. Neuroendocrinology. In: Jankovic J, Mazziotta JC, Pomeroy SL, Newman NJ, eds. Bradley and Daroff's Neurology in Clinical Practice. 8th ed. Philadelphia, PA: Elsevier; 2022:chap 50. Melmed S, Casanueva FF. Pituitary adenomas and masses. In: Melmed S, Auchus RJ, Goldfine AB, Rosen CJ, Kopp PA, eds. Williams Textbook of Endocrinology. 15th ed. Philadelphia, PA: Elsevier; 2025:chap 7. Weiss RE. Anterior pituitary. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 205. | ||
| ||
Review Date: 4/24/2025 Reviewed By: Sandeep K. Dhaliwal, MD, board-certified in Diabetes, Endocrinology, and Metabolism, Springfield, VA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


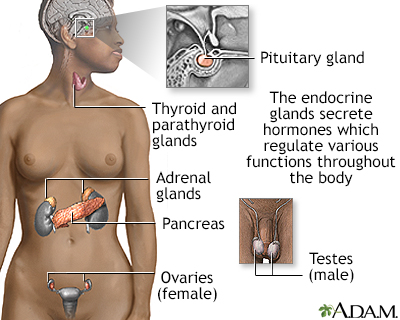 Endocrine glands
Endocrine glands