Somatotroph adenoma; Growth hormone excess; Growth hormone secreting pituitary adenoma; Pituitary giant (in childhood) DefinitionAcromegaly is a condition in which there is too much growth hormone (GH) in your body. CausesAcromegaly is a rare condition. It is caused when the pituitary gland makes too much GH. The pituitary gland is a small endocrine gland attached to the bottom of the brain. It regulates, makes, and releases several hormones, including GH. Usually, a noncancerous (benign) tumor of the pituitary gland releases too much GH. In rare cases, pituitary tumors can be inherited. In children, too much GH causes gigantism rather than acromegaly. SymptomsSymptoms of acromegaly may include any of the following:
Other symptoms that may occur with this disease:
Exams and TestsYour health care provider will perform a physical exam and ask about your symptoms. The following tests may be ordered to confirm the diagnosis of acromegaly and check for complications:
Other tests may be ordered to check whether the rest of the pituitary gland is working normally. Often a GH suppression test is needed. This involves drawing blood from a vein 4 or 5 times over 2 hours before and after drinking a specific amount of a sugar solution. Glucose and GH are measured in the blood. TreatmentSurgery to remove the pituitary tumor that is causing this condition often corrects the abnormal GH level. Sometimes, the tumor is too large to be removed completely and acromegaly is not cured. In this case, medicines and radiation (radiotherapy) may be used to treat acromegaly. Some people with tumors that are too complicated to remove by surgery are treated with medicines instead of surgery. These medicines may block the production of GH from the pituitary gland or prevent the action of GH in other parts of the body. After treatment, you will need to see your provider regularly to make sure that the pituitary gland is working normally and that acromegaly does not come back. Yearly evaluations are usually recommended. Support GroupsMore information and support for people with acromegaly and their families can be found at:
Outlook (Prognosis)Pituitary surgery is successful in most people, depending on the size of the tumor and the experience of the neurosurgeon with pituitary tumors. Without treatment, the symptoms will get worse. Conditions such as high blood pressure, diabetes, and heart disease may result. Possible ComplicationsSurgery and radiation treatment may lead to low levels of other pituitary hormones. This can cause any of the following conditions:
When to Contact a Medical ProfessionalContact your provider if:
PreventionAcromegaly cannot be prevented. Early treatment may prevent the disease from getting worse and help to avoid complications. ReferencesBiondi B. Endocrine disorders and cardiovascular disease. In: Libby P, Bonow RO, Mann DL, Tomaselli GF, Bhatt DL, Solomon SD, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 12th ed. Philadelphia, PA: Elsevier; 2022:chap 96. Katznelson L, Laws ER Jr, Melmed S, et al. Acromegaly: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2014;99(11):3933-3951. PMID: 25356808 pubmed.ncbi.nlm.nih.gov/25356808/. Lebovitz HE. Hyperglycemia secondary to non-traditional diabetic conditions. In: Robertson RP, ed. DeGroot's Endocrinology. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 35. Melmed S, Casanueva FF. Pituitary adenomas and masses. In: Melmed S, Auchus RJ, Goldfine AB, Rosen CJ, Kopp PA, eds. Williams Textbook of Endocrinology. 15th ed. Philadelphia, PA: Elsevier; 2025:chap 7. Weiss RE. Anterior pituitary. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 205. | ||
| ||
Review Date: 4/24/2025 Reviewed By: Sandeep K. Dhaliwal, MD, board-certified in Diabetes, Endocrinology, and Metabolism, Springfield, VA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


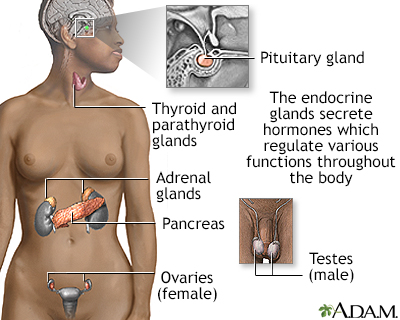 Endocrine glands
Endocrine glands