Primary biliary cirrhosis (the old name for the disease); PBC DefinitionThe bile ducts are tubes that move bile from the liver to the small intestine. Bile is a substance that helps with digestion. All of the bile ducts together are called the biliary tract. When the bile ducts become swollen or inflamed, this blocks the flow of bile. These changes can lead to scarring of the liver called cirrhosis. This is called biliary cirrhosis. Advanced cirrhosis can lead to liver failure. CausesThe cause of inflamed bile ducts in the liver is not known. However, primary biliary cholangitis is an autoimmune disorder. That means your body's immune system mistakenly attacks healthy tissue. The disease may be linked to autoimmune disorders such as:
The disease most often affects middle-aged women. SymptomsMore than one half of people have no symptoms at the time of diagnosis. Symptoms most often begin slowly. Early symptoms may include:
As liver function worsens, symptoms may include:
Exams and TestsThe health care provider will do a physical exam. The following tests can check to see if your liver is working properly:
Other tests that can help measure how severe liver disease may be include:
TreatmentThe goal of treatment is to ease symptoms and prevent complications. Cholestyramine (or colestipol) may reduce the itching. Ursodeoxycholic acid may improve removal of bile from the bloodstream. This may improve survival in some people. A newer drug called obeticholic acid (Ocaliva) is also available. Vitamin replacement therapy restores vitamins A, K, E and D, which are lost in the fatty stools that may occur in people with primary biliary cholangitis. A calcium supplement or other bone medicines may be added to prevent or treat weak or soft bones. Long-term monitoring and treatment of liver failure is needed. Liver transplant may be successful if it is done before liver failure occurs. Outlook (Prognosis)The outcome can vary. If the condition is not treated, most people will die without a liver transplant. About one quarter of people who have had the disease for 10 years will have liver failure. Doctors can now use a statistical model to predict the best time to do the transplant. Other diseases, such as hypothyroidism and anemia, can also develop. DEXA scans for bone health are checked regularly. Possible ComplicationsProgressive cirrhosis can lead to liver failure. Complications can include:
When to Contact a Medical ProfessionalContact your provider if you have:
ReferencesEaton JE, Lindor KD. Primary biliary cholangitis. In: Feldman M, Friedman LS, Brandt LJ, eds. Sleisenger and Fordtran's Gastrointestinal and Liver Disease. 11th ed. Philadelphia, PA: Elsevier; 2021:chap 91. Fogel EL, Sherman S. Diseases of the gallbladder and bile ducts. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 141. Garcia-Tsao G. Cirrhosis and its sequelae. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 139. Lamps LW. Liver: non-neoplastic diseases. In: Goldblum JR, Lamps LW, McKenney JK, Myers JL, eds. Rosai and Ackerman's Surgical Pathology. 11th ed. Philadelphia, PA: Elsevier; 2018:chap 19. | ||
| ||
Review Date: 6/11/2024 Reviewed By: Jenifer K. Lehrer, MD, Department of Gastroenterology, Aria - Jefferson Health Torresdale, Jefferson Digestive Diseases Network, Philadelphia, PA. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


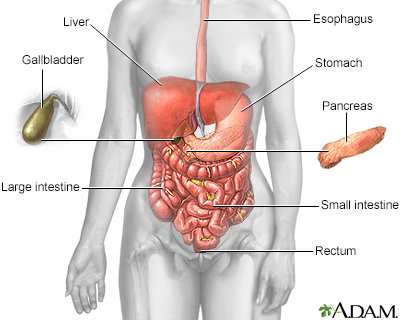 Digestive system
Digestive system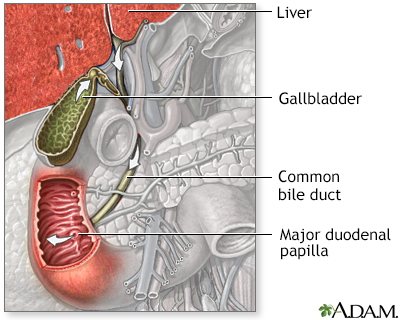 Bile pathway
Bile pathway