IBS; Irritable bowel; Spastic colon; Irritable colon; Mucous colitis; Spastic colitis; Abdominal pain - IBS; Diarrhea - IBS; Constipation - IBS; IBS-C; IBS-D DefinitionIrritable bowel syndrome (IBS) is a disorder that leads to pain in abdomen and changes in bowel movements. IBS is not the same as inflammatory bowel disease (IBD). CausesThe reasons why IBS develops are not clear. It can occur after a bacterial infection or a parasitic infection (such as giardiasis) of the intestines. This is called postinfectious IBS. There may also be other triggers, including stress. The intestine is connected to the brain by hormone and nerve signals that go back and forth between the bowel and the brain. These signals affect bowel function and symptoms. The nerves can become more active during stress. This can cause the intestines to be more sensitive and contract more. IBS can occur at any age. Often, it begins in the teen years or early adulthood. It is twice as common in women as in men. It is less likely to begin in people above 50 years of age. About 10% to 15% of people in the United States have symptoms of IBS. It is the most common intestinal problem that causes people to be referred to a bowel specialist (gastroenterologist). SymptomsIBS symptoms vary from person to person, and range from mild to severe. Most people have mild symptoms. You are said to have IBS when symptoms are present for at least 3 days a month for a period of 3 months or more. The main symptoms include:
Pain and other symptoms will often be reduced or go away after a bowel movement. The pain should not occur when you are sleeping, and should not wake you up from sleep. Symptoms may flare up when there is a change in the frequency of your bowel movements. People with IBS may go back and forth between having constipation and diarrhea or have or mostly have one or the other. This is called mixed irritable bowel syndrome, or IBS-M.
The symptoms may get worse for a few weeks or a month, and then decrease for a while. In other cases, symptoms are present most of the time. You may also lose your appetite if you have IBS. However, blood in stools and unintentional weight loss are not a part of IBS. If you have these symptoms, you should work with your health care provider to find out why. Exams and TestsThere is no test to diagnose IBS. Most of the time, your provider can diagnose IBS based on your symptoms. Eating a lactose-free diet for 2 weeks may help your provider identify lactose intolerance that may be due to lactase deficiency. The following tests may be done to check for other problems:
Your provider may recommend a colonoscopy. During this test, a flexible tube is inserted through the anus to examine the colon. You may need this test if:
Other disorders that can cause similar symptoms include:
TreatmentThe goal of treatment is to relieve symptoms. In some people with IBS, lifestyle changes can help. For example, regular exercise and improved sleep habits may reduce anxiety and help relieve bowel symptoms. Dietary changes can be helpful. However, no specific diet can be recommended for IBS because the condition differs from one person to another. The following changes may help:
Talk with your provider before taking over-the-counter medicines. No one medicine works for everyone. Some that your provider may suggest include:
Psychological therapy or medicines for anxiety or depression may help with the problem. Outlook (Prognosis)IBS may be a life-long condition. For some people, symptoms are disabling and interfere with work, travel, and social activities. Symptoms often get better with treatment. IBS does not cause permanent harm to the intestines. Also, it does not lead to a serious disease, such as cancer. When to Contact a Medical ProfessionalContact your provider if you have symptoms of IBS or if you notice changes in your bowel habits that do not go away. ReferencesAronson JK. Laxatives. In: Aronson JK, ed. Meyler's Side Effects of Drugs. 16th ed. Waltham, MA: Elsevier; 2016:488-494. Chang L. Irritable bowel and functional upper gastrointestinal syndromes. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 123. Ford AC, Talley NJ. Irritable bowel syndrome. In: Feldman M, Friedman LS, Brandt LJ, eds. Sleisenger and Fordtran's Gastrointestinal and Liver Disease. 11th ed. Philadelphia, PA: Elsevier; 2021:chap 122. Waller DG. Constipation, diarrhoea and irritable bowel syndrome. In: Waller DG, ed. Medical Pharmacology and Therapeutics. 6th ed. Philadelphia, PA: Elsevier; 2022:chap 35. | ||
| ||
Review Date: 4/21/2025 Reviewed By: Todd Eisner, MD, Private practice specializing in Gastroenterology in Boca Raton and Delray Beach, Florida at Gastroenterology Consultants of Boca Raton. Affiliate Assistant Professor, Florida Atlantic University School of Medicine. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


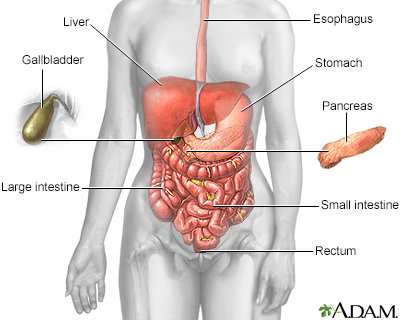 Digestive system
Digestive system