  |
 Pre-eclampsia video |
Pre-eclampsia
Pre-eclampsia is a form of high blood pressure associated with protein in the urine that is brought on by pregnancy. It is also known as toxemia. Eclampsia develops in women who have seizures or convulsions caused by a severe form of pre-eclampsia.
Because it causes your blood vessels to constrict, pre-eclampsia reduces the amount of oxygen and nutrients delivered to your baby and can lead to low birth weight. Left untreated, it can also cause your liver, lungs, and kidneys to fail. Despite intensive research, no one knows exactly what causes this condition, and it continues to affect roughly 7 out of 100 pregnant women. Humans are the only species that are known to get this disease, so animal research has not been helpful.
Pre-eclampsia appears during the second half of pregnancy, and is more likely to show up in first pregnancies, multiple births, teenagers, and women over 35. Less commonly, pre-eclampsia can occur in the first week after delivery. If you have chronic high blood pressure, a kidney disorder, or diabetes, you are at higher risk for pre-eclampsia. If you've had the disorder before, the odds are 25% to 50% that you'll develop it in a future pregnancy as well. If your mother had the disorder you are also at increased risk. Those with the angiotensinogen gene T235 have 20 times the average risk of developing this condition.
Eclampsia is much less common, afflicting only one in 1,500 pregnant women. Eclampsia and the severe form of pre-eclampsia called the HELLP syndrome are thought to be caused by untreated pre-eclampsia. Eclampsia results in convulsions that can put both you and your baby at risk. In very rare cases, eclampsia is fatal. If you get early, regular prenatal care, though, pre-eclampsia can be caught and treated, with little risk of progressing to eclampsia.
How Do I Know Have It?
If you have mild pre-eclampsia, you may not notice any symptoms at all. But during each prenatal visit, your health care provider will measure your blood pressure, test your urine, and be on the lookout for other early signs of the disease - a good reason not to miss any of your checkups.
Signs of pre-eclampsia include:
- Blood pressure of 140/90 or higher at two separate occasions at least 6 hours apart
- Protein in your urine
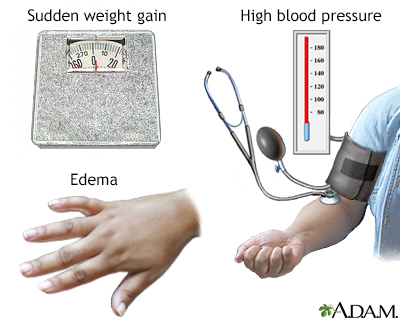
The symptoms of severe pre-eclampsia are more obvious. They include:
- Constant, severe headaches
- Blurred vision or spots in front of your eyes (called scotomata)
- Sensitivity to light
- Lethargy
- Nausea and vomiting
- Severe swelling
- Sudden weight gain of more than a pound a day
- Pain in the upper right side of your abdomen
- Shortness of breath
- Brisk reflexes (called hyperreflexia)
If pre-eclampsia isn't brought under control, the disease may progress to eclampsia. As pre-eclampsia worsens your urine protein may get progressively worse, you may have abnormal liver function tests, and your urine output may slow down (oliguria).
Eclampsia may involve any of the features of pre-eclampsia, along with:
- Convulsions
- Unconsciousness or coma
How Is Pre-eclampsia Treated?
The treatment for pre-eclampsia is delivery. So if the disease is mild and you're within a few weeks of your due date, your doctor will induce labor. If you develop pre-eclampsia before your baby can be safely delivered, your doctor may recommend bed rest at home or in the hospital, and may receive antihypertensive medications to bring your blood pressure under control.
Your physician will also follow you closely by performing medical tests to see if your condition may be worsening. These tests may include a blood count to check for low platelets, a blood test of kidney function, or a 24-hour collection of urine to accurately determine how much protein you are putting out of your kidneys. Liver or kidney dysfunction is a sign of deterioration that could prompt your physician to deliver the baby early. If you are less than 34 weeks pregnant, you may be a candidate for a steroid injection to mature the lungs. If your physician is uncertain if you need this treatment, an amniocentesis can be done to determine the maturity of your baby's lungs. If your baby’s lungs are not yet mature, you may have to check into the hospital for complete bed rest and observation, which allows the baby more time to mature. If your condition worsens or your baby shows signs of trouble, though, labor will be induced right away.
It’s important to understand that the cure for pre-eclampsia is delivery. If you and your doctor decide to wait to allow the baby to mature, then you are taking on the risk of added complications in an effort to help your baby.
In severe cases, since the only known treatment is delivery, your doctor will induce labor regardless of your due date, since the risks of pre-eclampsia (kidney failure, severe bleeding, and eclampsia) outweigh the risks of premature delivery. She may also give you intravenous magnesium sulfate to prevent eclamptic seizures.
If you have eclampsia, immediate delivery is required. Your doctor will give you intravenous magnesium sulfate to control the seizures and may give you antihypertensive medication to lower your blood pressure.
After delivery, your doctor will monitor you closely and may keep you on antiseizure medication for a day or so. In almost all women, the symptoms of pre-eclampsia lessen a day or two after birth and vanish entirely within a week. Women with severe disease may go home with blood pressure medication for the first few weeks after delivery. If your blood pressure hasn't returned to normal by your six-week checkup, your doctor will look for other problems, such as a liver, blood, or kidney disorder.
How Can I Prevent It?
There is no known way to prevent pre-eclampsia, but with good prenatal care, you can catch the condition early and keep it under control. This involves seeing your caregiver often so she can keep tabs on your blood pressure and monitor the amount of protein in your urine.
Some studies show that taking low doses of aspirin every day may prevent pre-eclampsia from recurring. There is also some evidence that calcium may reduce the risk of pre-eclampsia in high-risk women. If you had pre-eclampsia in a previous pregnancy, talk to your doctor about whether this makes sense for you.
Frequently Asked Questions (FAQ)
Q: If I develop pre-eclampsia during pregnancy, will I continue to have high blood pressure after giving birth?
A: It depends. Women who develop pre-eclampsia close to their due date do not seem to have higher risk of blood pressure problems in the future. By contrast, women with early onset pre-eclampsia have an increased risk of heart problems and high blood pressure.
Q: I'm pregnant and my doctor says my blood pressure is high. Does this mean I have pre-eclampsia?
A: Not necessarily. Pre-eclampsia is almost always accompanied by other symptoms, such as protein in your urine and excessive swelling. Your doctor will continue to monitor your blood pressure and watch out for these symptoms. If they don't develop, then you probably won't get pre-eclampsia.
If you start out your pregnancy with high blood pressure, then you are more at risk to develop pre-eclampsia than the general population.
Q: Will cutting out salt lower my chances of developing pre-eclampsia?
A: No. While too much sodium is never good, you need salt to help promote the flow of fluid in your body. Talk to your doctor about how much salt is safe to consume during pregnancy.
Reviewed By: Irina Burd, MD, PhD, Maternal Fetal Medicine, Johns Hopkins University, Baltimore, MD. Review provided by VeriMed Healthcare Network.
© 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
 All rights reserved.
All rights reserved.