Amyloidosis - cardiac; Primary cardiac amyloidosis - AL type; Secondary cardiac amyloidosis - AA type; Stiff heart syndrome; Senile amyloidosis DefinitionCardiac amyloidosis is a disorder caused by deposits of an abnormal protein (amyloid) in the heart tissue. These deposits make it hard for the heart to work properly. CausesAmyloidosis is a group of diseases in which clumps of proteins called amyloid build up in body tissues. Over time, these proteins replace normal tissue, leading to failure of the involved organ. There are many forms of amyloidosis. Cardiac amyloidosis ("stiff heart syndrome") occurs when amyloid deposits take the place of normal heart muscle. It is the most typical type of restrictive cardiomyopathy. Cardiac amyloidosis may affect the way electrical signals move through the heart (conduction system). This can lead to abnormal heartbeats (arrhythmias) and faulty heart signals (heart block). The condition can be inherited. This is called familial cardiac amyloidosis. It can also develop as the result of another disease such as a type of bone and blood cancer, or as the result of another medical problem causing inflammation. Cardiac amyloidosis is more common in men than in women. The disease is rare in people under age 40. SymptomsSome people may have no symptoms. When present, symptoms may include:
Exams and TestsThe signs of cardiac amyloidosis can be related to a number of different conditions. This can make the problem hard to diagnose. Signs may include:
The following tests may be done:
An ECG may show problems with the heartbeat or heart signals. It may also show low signals (called "low voltage"). A cardiac biopsy may be used to confirm the diagnosis. A biopsy of another area, such as the abdomen, kidney, or bone marrow, is often done as well. TreatmentYour health care provider may tell you to make changes to your diet, including limiting salt and fluids. You may need to take water pills (diuretics) to help your body get rid of excess fluid. Your provider may tell you to weigh yourself every day. A weight gain of 3 or more pounds (1 kilogram or more) over 1 to 2 days can mean there is too much fluid in the body. Medicines including digoxin, calcium-channel blockers, and beta-blockers may be used in people with atrial fibrillation. However, the medicines must be used with caution, and the dosage must be carefully monitored. People with cardiac amyloidosis may be extra sensitive to side effects of these medicines. Other treatments may include:
A heart transplant may be considered for people with some types of amyloidosis who have very poor heart function. People with hereditary amyloidosis may need a liver transplant. Outlook (Prognosis)In the past, cardiac amyloidosis was thought to be an untreatable and rapidly fatal disease. However, the field is changing rapidly. Different types of amyloidosis can affect the heart in different ways. Some types are more severe than others. Many people can now expect to survive and experience a good quality of life for several years after diagnosis. Possible ComplicationsComplications may include:
When to Contact a Medical ProfessionalContact your provider if you have this disorder and develop new symptoms such as:
ReferencesElliott PM, Olivotto I. Diseases of the myocardium and endocardium. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 47. Hershberger RE. The dilated, restrictive, and infiltrative cardiomyopathies. In: Libby P, Bonow RO, Mann DL, Tomaselli GF, Bhatt DL, Solomon SD, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 12th ed. Philadelphia, PA: Elsevier; 2022:chap 52. | ||
| ||
Review Date: 5/8/2024 Reviewed By: Thomas S. Metkus, MD, Assistant Professor of Medicine and Surgery, Johns Hopkins University School of Medicine, Baltimore, MD. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


 Heart - section th...
Heart - section th...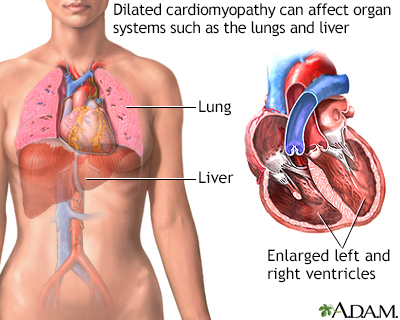 Dilated cardiomyop...
Dilated cardiomyop...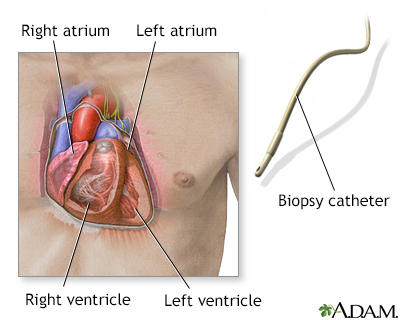 Biopsy catheter
Biopsy catheter