Aneurysm - aortic; AAA DefinitionThe aorta is the main blood vessel that supplies blood to the abdomen, pelvis, and legs. An abdominal aortic aneurysm (AAA) occurs when an area of the aorta in the abdomen becomes very large or balloons out. CausesThe exact cause of an aneurysm is unknown. It occurs due to weakness in the wall of the artery. Factors that can increase your risk of having this problem include:
An abdominal aortic aneurysm is most often seen in males over age 60 who have one or more risk factors. The larger the aneurysm, the more likely it is to break open or tear. This can be life threatening. SymptomsAneurysms can develop slowly over many years, often with no symptoms. Symptoms may come on quickly if the aneurysm expands rapidly, tears open or leaks blood within the wall of the vessel (aortic dissection). Symptoms of rupture include:
Exams and TestsYour health care provider will examine your abdomen and feel the pulses in your legs. The provider may find:
Your provider may find this problem by doing the following tests:
Any one of these tests may be done when you are having symptoms. You may have an abdominal aortic aneurysm that is not causing any symptoms. Your provider may order an ultrasound of the abdomen to screen for an aneurysm.
TreatmentIf you have bleeding inside your body from an aortic aneurysm, you will need surgery right away. If the aneurysm is small and there are no symptoms:
Most of the time, surgery is done if the aneurysm is bigger than 2 inches (5 centimeters) across or growing quickly. The goal is to do surgery before complications develop. There are two types of surgery:
Outlook (Prognosis)The outcome is often good if you have surgery to repair the aneurysm before it ruptures. When an abdominal aortic aneurysm begins to tear or ruptures, it is a medical emergency. Only about 1 in 5 people survive a ruptured abdominal aneurysm. When to Contact a Medical ProfessionalGo to the emergency room or call 911 or the local emergency number if you have pain in your belly or back that is very bad or does not go away. PreventionTo reduce the risk of aneurysms:
People over age 65 who have ever smoked should have a screening ultrasound done once. ReferencesBraverman AC, Schermerhorn M. Diseases of the aorta. In: Libby P, Bonow RO, Mann DL, Tomaselli GF, Bhatt DL, Solomon SD, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 12th ed. Philadelphia, PA: Elsevier; 2022:chap 42. Colwell CB. Abdominal aortic aneurysm. In: Walls RM, ed. Rosen's Emergency Medicine: Concepts and Clinical Practice. 10th ed. Philadelphia, PA: Elsevier; 2023:chap 72. Isselbacher EM, Preventza O, Black JH 3rd, et al. 2022 ACC/AHA Guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;80(24) e223–e393. PMID: 36334952 pubmed.ncbi.nlm.nih.gov/36334952/. Owens DK, Davidson KW, Krist AH, et al. Screening for abdominal aortic aneurysm: US Preventive Services Task Force Recommendation Statement. JAMA. 2019;322(22):2211-2218. PMID: 31821437 pubmed.ncbi.nlm.nih.gov/31821437/. Sharafuddin MJ. Abdominal aortic aneurysms: open surgical treatment. In: Sidawy AN, Perler BA, eds. Rutherford's Vascular Surgery and Endovascular Therapy. 10th ed. Philadelphia, PA: Elsevier; 2023:chap 73. | ||
| ||
Review Date: 8/22/2023 Reviewed By: Mary C. Mancini, MD, PhD, Cardiothoracic Surgeon, Shreveport, LA. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


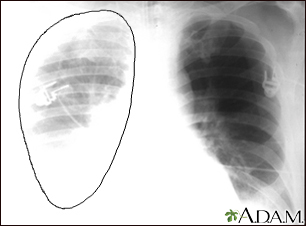 Aortic rupture - c...
Aortic rupture - c...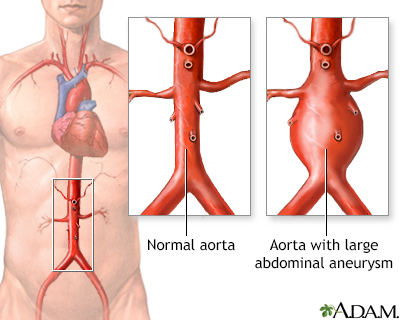 Aortic aneurysm
Aortic aneurysm