Formerly: Wegener's granulomatosis DefinitionGranulomatosis with polyangiitis (GPA) is a rare disorder in which blood vessels become inflamed. This leads to damage in major organs of the body. It was formerly known as Wegener's granulomatosis. CausesGPA mainly causes inflammation of blood vessels in the lungs, kidneys, nose, sinuses, and ears. This is called vasculitis or angiitis. Other areas may also be affected in some cases. The disease can be fatal and prompt treatment is important. In most cases, the exact cause is not known, but it is an autoimmune disorder. Rarely, vasculitis with positive antineutrophil cytoplasmic antibodies (ANCA) has been caused by several drugs including cocaine cut with levamisole, hydralazine, propylthiouracil, and minocycline. GPA is most common in middle-aged adults of northern European descent. It is rare in children. SymptomsFrequent sinusitis and bloody noses are the most common symptoms. Other early symptoms include a fever that has no clear cause, night sweats, fatigue, and a general ill feeling (malaise). Other common symptoms may include:
Less common symptoms include:
Exams and TestsYou may have a blood test that looks for ANCA proteins as well as two additional proteins called proteinase 3 (PR3) and myeloperoxidase (MPO). These tests are abnormal in most people with active GPA, however, this test is sometimes negative, even in people with the condition. A chest x-ray will be done to look for signs of lung disease. Urinalysis is done to look for signs of kidney disease, such as protein and blood in the urine. Sometimes urine is collected over 24 hours to check how the kidneys are working. Standard blood tests include:
Blood tests may be done to check for other illnesses. These may include:
A biopsy is sometimes needed to confirm the diagnosis and check how severe the disease is. A kidney biopsy is most commonly done. You may also have one of the following:
Other tests that may be done include:
TreatmentBecause of the potentially serious nature of GPA, you may be hospitalized. Once the diagnosis is made, you will probably be treated with high doses of glucocorticoids (such as prednisone). These are given through the vein for 3 to 5 days at the beginning of treatment. Prednisone is given along with other medicines that slow down the immune response. For milder disease other medicines that slow down the immune response such as methotrexate or azathioprine may be used. Common medicines for vasculitis include:
These medicines are effective in severe disease, but they may cause serious side effects. Most people with GPA are treated with ongoing medicines to prevent relapse for at least 12 to 24 months. Talk to your health care provider about your treatment plan. Other medicines used for GPA include:
Support GroupsSupport groups with others who suffer from similar diseases may help people with the condition and their families learn about the diseases and adjust to the changes associated with the treatment. Outlook (Prognosis)Without treatment, people with severe forms of this disease can die within a few months. With treatment, the outlook for most patients is good. Most people who receive corticosteroids and other medicines that slow the immune response get much better. Most people with GPA are treated with ongoing medicines to prevent relapse for at least 12 to 24 months. Possible ComplicationsComplications most often occur when the disease is not treated. People with GPA develop tissue damage in the lungs, airways, and the kidneys. Kidney involvement may result in blood in the urine and kidney failure. Kidney disease can quickly get worse. Kidney function may not improve, even when the condition is controlled by medicines. If untreated, kidney failure and possibly death occur in most cases. Other complications may include:
When to Contact a Medical ProfessionalContact your provider if:
PreventionThere is no known prevention. ReferencesHellmich B, Sanchez-Alamo B, Schirmer JH, et al. EULAR recommendations for the management of ANCA-associated vasculitis: 2022 update. Ann Rheum Dis. 2024;83(1):30-47. PMID: 36927642 pubmed.ncbi.nlm.nih.gov/36927642/. Stone JH. The systemic vasculitides. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 249. | ||
| ||
Review Date: 12/31/2023 Reviewed By: Neil J. Gonter, MD, Assistant Professor of Medicine, Columbia University, NY and private practice specializing in Rheumatology at Rheumatology Associates of North Jersey, Teaneck, NJ. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. View References The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | ||
| ||


 Granulomatosis wit...
Granulomatosis wit...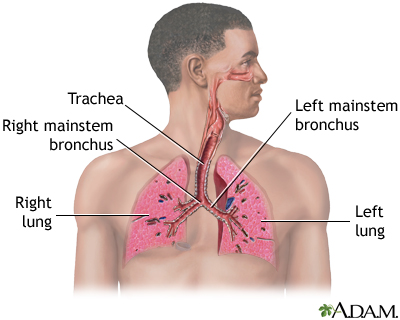 Respiratory system
Respiratory system