

Birth control options for women - InDepth
Highlights
Birth Control Options
Birth control options for women include:
- Hormonal contraceptives, such as birth control pills, skin patch, vaginal ring, injection, implant
- Intrauterine devices (IUDs), which contain either a hormone or copper
- Barrier devices, such as condoms, diaphragm, cervical cap, sponge
- Fertility awareness methods
- Sterilization
The condom is the only form of birth control that protects against most sexually transmitted diseases.
Emergency Contraception
Women of all ages can now get the levonorgestrel emergency contraceptive pill Plan B One-Step and its generic versions without a prescription. The other type of "morning-after pill", ulipristal (ella), requires a prescription. For some patients, an intrauterine device may be a good choice for emergency contraception.
Birth Control Pills and Blood Clots
All birth control pills containing estrogen can increase the risk for blood clots. For this reason, they are not recommended for women who have high blood pressure, a history of heart disease, are over age 35 and smoke, or who have other risk factors. So-called progestin-only birth control pills may not increase the risk of blood clots, though further studies are needed to clarify their risk. According to the Food and Drug Administration (FDA), birth control pills that contain drospirenone have a higher risk for causing blood clots than levonorgestrel or other types of progestin, although even with the increased risk, the total risk is still low.
It is important to know that pregnancy also increases the risk for blood clots, and much more significantly than any hormonal contraceptive.
IUDs and Implants for Adolescents
The American Academy of Pediatrics and the American College of Obstetricians and Gynecologists (ACOG) recommend intrauterine devices (IUDs) and contraceptive implants (Nexplanon) as first-line contraceptive options for sexually active teens based on the effectiveness of these contraceptives and high rates of patient satisfaction.
Introduction
Contraceptives are devices, drugs, or methods for preventing pregnancy either by preventing the fertilization of the female egg by the male sperm or by preventing implantation of the fertilized egg.
Contraceptive Options
Contraceptive options include:
- Hormonal contraceptives (such as oral contraceptives, skin patch, vaginal ring, implant, and injection)
- Intrauterine devices (IUDs), which contain either a hormone or copper
- Barrier devices with or without spermicides (such as diaphragm, cervical cap, sponge, and condom)
- Fertility awareness methods (such as temperature, cervical mucus, calendar, and symptothermal)
All of these methods are reversible. Permanent methods of birth control are tubal ligation for women, and vasectomy for men.
Emergency contraception is also included in this report. It is an option for situations when other birth control methods were not available or failed. It should not be used or substituted for regular birth control.
Considerations
Choosing the appropriate contraceptive is a personal decision. Here are some questions to consider when selecting a birth control method:
- How well does the method prevent pregnancy? To tell how well a method works, look at the number of pregnancies in 100 women using that method over a period of 1 year.
- How much does a method of birth control cost? Does your insurance plan pay for it
- What are the health risks? Do you have any medical conditions or lifestyle practices that may make a birth control method risky or difficult? Discuss the risks and benefits of birth control options with your health care provider.
- Do you want a method that you only need to use when you have sex? Or do you want something that is in place and always working?
- Do you want a method that is long lasting, reversible, and always in place? That doesn't require any action by you to be effective?
- How easily available is the method? Can you obtain it without a prescription, a provider visit or, in the case of minors, parental consent?
- How easily reversible is the method if you decide you want to get pregnant? How long will it take to regain your fertility after stopping birth control?
- What are your feelings about getting pregnant? Would an unplanned pregnancy create hardship or distress for you or your partner? Or would a pregnancy be welcomed if it occurred earlier than planned?
- Is your partner willing to accept and use a given method of birth control?
Condoms are the only birth control method that also protects against sexually transmitted infections (STIs), including HIV. However, they may not protect you against Human papilloma Virus (HPV). Condoms can be used along with another birth control method. Unless they have a monogamous relationship with an uninfected partner, all women should be sure to use a condom during sexual intercourse.
Effectiveness
Contraceptive effectiveness is characterized by "typical use" and "perfect use":
- Typical use refers to real-life conditions, in which mistakes (forgetting to take a birth control pill at the right time) sometimes happen.
- Perfect use refers to contraceptives that are used correctly each time.
The most effective birth control methods have a failure rate of less than 1% with typical (normal) use, which means they are nearly 100% effective. They are:
- Intrauterine devices (IUDs)
- Progestin implants
- Tubal sterilization
By comparison, the male latex condom is about 82% effective with typical use and 98% with perfect use. Birth control pills are about 91% effective with typical use and up to 99% effective with perfect use.
To put these rates into perspective, a sexually active woman of reproductive age who does not use contraception faces an 85% chance of becoming pregnant in the course of a year.
Oral Contraceptives (Birth Control Pills)
Oral contraceptives are also called OCs, birth control pills, or simply "the Pill." They are available by prescription and come in either a combination of estrogen and progestin or progestin alone.
Most women use the combination hormone pill. Women who experience severe headaches or high blood pressure from the estrogen in the combined pill can take the progestin-only pill (called a "mini-pill.")
The estrogen compound used in most combination birth control pills is ethinyl estradiol. There are many different progestins, but common types include levonorgestrol, drospirenone, norgestrol, norethindrone, and desogestrel.
Birth control pills work by:
- Preventing ovulation. Ovulation is the release of the egg from an ovary. If no egg is released, fertilization by sperm cannot occur.
- Preventing entry of sperm into the uterus by keeping the cervical mucus thick and sticky.
When a woman stops taking the pill, she usually regains fertility within 1 to 6 months.
Dosing and Pill Packs
Women who take birth control pills need to be sure to take the pills every day. It is best to get in the habit of taking the pill at the same time every day. Your risk for becoming pregnant if you miss a dose depends on the type of pill you are taking. Progestin-only pills have a stricter schedule than combination hormone pills.
For 28-day or 21-day combination OCs, catch-up doses depend on when in the cycle you forgot to take the pill. Read the directions that come with your pills and check with your health care provider or pharmacist if you have any questions. It is a good idea to keep on hand a back-up form of barrier birth control (condom, spermicide, sponge). Emergency ("morning after") contraception is another option.
Standard OCs
Traditional combination birth control pills come in either a:
- 28-pill pack with 21 days of "active" (hormone) pills and 7 days of "inactive" (placebo) pills.
- 21-pill pack with 21 days of "active" pills. You wait 7 days and then begin a new pack.
Continuous-Dosing OCs
Extended-cycle (also called "continuous-use" or "continuous-dosing") oral contraceptives aim to reduce or eliminate monthly menstrual periods. These OCs contain a combination of estradiol and the progestin levonorgestrel, but they use extending dosing of active pills with 81 to 84 days of active pills followed by 7 days of inactive or low-dose pills. Some types of continuous-dosing OCs use only active pills, which are taken 365 days a year.
Progestin-Only Pills
Progestin-only pills ("mini-pills") come in 28-pill pack that contains all active pills. Progestin-only pills must be taken at precisely the same time each day. You can become pregnant if you delay taking a pill by even 3 hours.
Advantages of Birth Control Pills
Oral contraceptives are about 91% effective with typical use (sometimes missing a dose). This means that about 9 in 100 women become pregnant each year while on birth control pills.
In addition to preventing pregnancy, oral contraceptives may also have the following advantages:
- Reduce heavy menstrual bleeding and cramping, which are often symptoms of uterine fibroids and endometriosis.
- Reduce pelvic pain caused by endometriosis.
- Help protect against endometrial and ovarian cancer with long-term use (1 or more years).
- Reduce symptoms of premenstrual dysphoric disorder associated with premenstrual syndrome.
- Improve acne.
- Reduce the risk of anemia (low blood count).
Disadvantages of Birth Control Pills
Side Effects
The hormones used in birth control pills can cause temporary side effects during the first 2 to 3 months of use. Common side effects of oral contraceptives include:
- Bleeding between periods
- Breast tenderness
- Nausea and vomiting
- Headaches (in women with a history of migraines, they may worsen)
Although women are often concerned about weight gain, most studies have not found this to be a side effect associated with oral contraceptives. The estrogen in combination birth control pills may cause some fluid retention.
Serious Risks
Combination birth control pills can increase the risk of developing or worsening certain serious medical conditions. The risks depend in part on a woman's medical history.
Birth control pills are not recommended for women who:
- Are over age 35 and smoke
- Have uncontrolled high blood pressure
- Have a history of heart disease, stroke, or blood clots or heart disease risk factors (unhealthy cholesterol levels, obesity)
- Have migraine with aura
- Have liver problems such as hepatic adenoma
Serious risks of birth control pills may include:
Venous Thromboembolism (VTE).
Combination estrogen/progestin birth control products increase the risk for blood clots in the veins (venous thromboembolism), which can lead to blood clots in the arteries of the leg (deep vein thrombosis) or lungs (pulmonary embolism). Drospirenone (found in brands such as Yaz) may increase the risk for blood clots more than other types of progestins.Heart and Circulation Problems.
Combination birth control pills contain estrogen, which can increase the risk for stroke, heart attack, and blood clots in some women. Your provider should screen you for high blood pressure before prescribing oral contraceptives.Cancer Risks.
Some studies suggest an association between increased risk of cervical cancer and long-term (greater than 5 years) use of oral contraception. However, it is not thought that the use of OCs actually causes cervical cancer, which is caused by exposure to the human papillomavirus. Recent research indicates that OCs do not significantly increase breast cancer risk.Drug Interactions.
Certain types of drugs can interact with and decrease the effectiveness of OCs. These medications include anticonvulsants, antibiotics, antifungals, and the herbal remedy St. John's wort. Make sure your provider is aware of any drugs, vitamins, or herbal supplements that you take.
Skin Patch and Vaginal Ring
The skin patch and vaginal ring are hormonal contraceptive methods of administering the combination of progestin and estrogen.
Skin Patch
The birth control skin patch (Ortho Evra, Xulane) contains a progestin (norelgestromin) and estrogen. Xulane is a generic version of the Ortho Evra brand. The patch is available by prescription.
The patch is placed on the lower abdomen, buttocks, or upper body (not on the breasts). Each patch is worn continuously for a week and reapplied on the same day of each week. After 3 weekly patches, the fourth week is patch-free, which allows menstruation. The patch remains effective for 9 days, so being slightly late in changing it does not increase the risk for pregnancy. When applying a new patch, place it in a different location than the previous patch.
The patch is about 91% effective with typical use. It may be less effective in women who weigh more than 198 pounds (89 kilograms).
Side Effects
The patch has side effects that are similar to birth control pills. These include bleeding between periods, breast tenderness, and nausea. The patch may cause skin irritation at the site where it is placed.
The patch exposes women to higher levels of estrogen than most birth control pills, and therefore has a higher risk for blood clots in the veins (venous thromboembolism). Venous thromboembolism (VTE) can cause blockage in lung arteries and other serious side effects. Due to the risks of VTE, women who smoke cigarettes and are over age 35 should not use the patch.
Vaginal Ring
NuvaRing is a prescription 2-inch flexible ring that contains both estrogen and progestin (etonogestrel). It is inserted into the vagina. You insert the ring once a month and take it out at the end of the third week to allow menstruation.
The ring may accidently slip out of the vagina during sexual intercourse or bowel movements. It can be reinserted.
The vaginal ring is about 92% effective with typical use. It may cause less irregular bleeding than oral contraceptives.
Side Effects
Side effects include vaginal infections, irritation, and discharge. As with the patch, NuvaRing contains a higher level of estrogen than birth control pills and may pose a higher risk for blood clots. It should not be used by women who smoke cigarettes and are over age 35.
Progestin Implant
Progestin implant contraception (Nexplanon) involves inserting a tiny rod, about the size of a matchstick, under the skin. The rod releases tiny amounts of the hormone progestin into the bloodstream. Etonogestrel is the type of progestin used in the implant.
Implant insertion takes about a minute and is performed with a local anesthetic in a health care provider's office. The rod remains in place for 3 years, although it can be removed at any time. (The removal procedure takes a few minutes longer than insertion.) After the rod is removed, a new one can be inserted.
Implants and intrauterine devices (IUDs) are long-acting reversible contraceptives (LARC), which are considered the most effective type of birth control. These methods are 20 times more effective than short-acting contraceptives like birth control pills.
Implant contraception is 99% effective with failure rates of less than 1%. The American College of Obstetricians and Gynecologists and the American Academy of Pediatrics recommend progestin implants or IUDs as first-line contraceptive options for adolescents.
The progestin implant is generally safe. Irregular bleeding and headaches are the main side effects. Although the risk for pregnancy is very low (fewer than 1 of 100 women), if conception does occur there is an increased chance for ectopic pregnancy, which is a dangerous condition. Implants can also increase the risks for ovarian cysts, and for blood clots.
Progestin Injection
Progestin injection (Depo-Provera) is given as a shot once every 3 months. Depo-Provera is also called Depo, or DMPA. The contraceptive uses a progestin called medroxyprogesterone. The injection slowly releases the hormone into your body.
A health care provider gives the injection into your upper arm or buttocks. You need to return to the provider's office every 12 weeks for a repeat shot. A lower-dose version of the shot (Depo-subQ Provera 104) is injected subcutaneously (under the skin).
The progestin injection is about 97% effective in preventing pregnancies. However, it may take up to 10 months after stopping injections before you will begin ovulating again. For this reason, progestin injections are not a good choice for women who hope to get pregnant within a year after stopping birth control.
The main side effects of progestin injection are:
- Irregular menstrual bleeding with fewer or lighter periods. After a year, about half of women who use these injections have no menstrual cycles.
- Breast tenderness and weight gain, headaches, or depression.
- Side effects may continue for 12 to 14 weeks after the shot.
A serious concern with progestin injections is that long-term use can cause loss of bone mineral density (bone strength). For this reason, injections should not be used for longer than 2 years unless other birth control methods are inadequate. The decline in bone density increases with duration of use and may not be completely reversible even after the drug is discontinued. Some studies indicate that this bone loss may be reversible once the injections are stopped.
The progestin injection should not be used by women who have a history of:
- Current or past breast cancer
- Stroke or blood clots
- Liver disease
- Unexplained vaginal bleeding
- Risk for osteoporosis
Intrauterine Devices (IUDs)
The intrauterine device (IUD) is a small plastic T-shaped device that is inserted into the uterus. An IUD's contraceptive action begins as soon as the device is placed in the uterus and stops as soon as it is removed. IUDs have an effectiveness rate of close to 100%. Once the device is removed, a woman quickly regains her fertility.
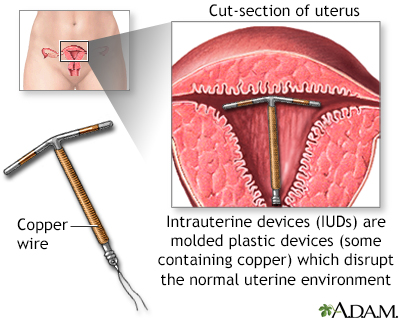
The intrauterine device (IUD) shown uses copper as the active contraceptive. Others use progesterone in a plastic device.
Types of Intrauterine Devices
Two types of intrauterine devices (IUDs) are available in the United States:
Copper-Releasing (ParaGard).
This type of IUD can remain in the uterus for up to 10 years. Copper ions released by the IUD are toxic to sperm, thus preventing fertilization. The copper-releasing IUD is also effective for emergency contraception. (See Emergency Contraception section of this report.)Progestin-Releasing (Mirena, Skyla).
This type of hormonal IUD is also known as a levonorgestrel-releasing intrauterine system, or LNG-IUS. Levonorgestrel is a progestin. Mirena is effective for contraception for 5 years, while Skyla is slightly smaller and can remain inserted for up to 3 years. Mirena is also approved as a treatment for heavy menstrual bleeding.
Inserting an Intrauterine Device
A health care provider inserts an IUD into a woman's uterus during an office visit. The insertion process takes a few minutes. The provider inserts a plastic applicator tube that contains the IUD and presses a plunger to release the IUD. The tube is then withdrawn.
The provider will check to make sure that the IUD is placed properly and that the strings attached to it hang outside the cervix within the vagina. The strings are used for removal.
Some women experience mild discomfort and cramps during the insertion procedure. Once the IUD is in place, neither you nor your partner will feel it. You can check the strings periodically (but do not tug them) to make sure the IUD is in place.
The copper IUD is immediately effective once it is inserted. A hormonal IUD takes about 7 days to become effective.
Advantages of IUDs
Intrauterine devices are nearly 100% effective.
An IUD has the following advantages:
- It is more effective than oral contraceptives at preventing pregnancy and, unlike the pill; there is no daily routine to follow.
- It is the least expensive form of contraception over the long term.
- IUDs and implant contraceptives are recommended as the best birth control methods for adolescents.
- If you wish to become pregnant, the IUD can easily be removed. You will regain your fertility within a few weeks.
Additional advantages of IUDs include:
- The progestin-releasing LNG-IUS (Mirena) is considered to be one of the best options for treating heavy menstrual bleeding. Most women experience fewer cramps and lighter periods. Some women stop bleeding altogether.
- The copper-releasing IUDs do not have hormonal side effects and may help protect against endometrial (uterine) cancer.
- Both types of IUDs may lower the risk of developing cervical cancer.
Disadvantages of IUDs
You should not get an IUD if you:
- Have had serious pelvic infections or pelvic inflammatory disease.
- Are at high risk for pelvic infections. Women who have multiple sex partners or who are in a non-monogamous relationship have an increased risk for infections.
- Have had cancer of the breast, uterus, or cervix.
Disadvantages of IUDs include:
- Side effects may include vaginal itching, abdominal or pelvic pain, acne, headache, nausea, and bloating.
- Copper-releasing IUDs can cause cramps, longer and heavier menstrual periods, and spotting between periods.
- Progestin-releasing IUDs may produce irregular bleeding and spotting during the first few months. Some women may experience heavier bleeding and cramps during this time. However, most women have light or no menstrual cycles after 6 months of use.
- IUDs may increase the risk for ovarian cysts.
- In rare cases conception does occur despite the presence of the IUD. If that happens, the fertilized egg may implant outside the uterus, a condition called ectopic pregnancy.
- In very rare cases, perforation (puncture) of the uterus can occur during insertion.
Sometimes an IUD can slip out and be expelled from the uterus. Expulsion is more likely to occur during the first year after insertion, and in younger women (ages 14 to 19). If you think your IUD has come out, use a back-up form of birth control and call your provider.
Spermicidal and Barrier Contraceptives
Barrier contraceptives provide a physical or chemical barrier to block sperm from passing through the cervix into the uterus and fertilizing the egg. Examples of barrier contraceptives include:
- Spermicides
- Condoms, which are the only type of contraception that protects against some sexually transmitted infections (STIs)
- Diaphragms and cervical caps
- Sponge
Spermicides
Spermicides are sperm-killing substances available as foams, creams, gels, films, or suppositories. They are typically used along with another barrier device. Diaphragms and cervical caps require the application of a spermicide to be effective. The sponge comes pre-applied with a spermicide. Some condoms come pre-lubricated with spermicide.
When used alone, the spermicide is inserted into the vagina within 30 minutes of sexual intercourse and must be reapplied every time you have sex.
Spermicides are relatively inexpensive and can be purchased at a drugstore without a prescription. In general, spermicides may be an appropriate choice for women who have intercourse only once in a while, or need backup protection against pregnancy (for instance, if they forget to take their birth control pills). They are not recommended as a primary form of birth control.
Spermicides have several disadvantages:
- Nonoxynol-9, the chemical in U.S.-made spermicides, does not provide any protection against sexually transmitted diseases. In fact, frequent use of nonoxynol-9 can cause vaginal and rectal irritation and abrasions that may increase the risk for HIV transmission in women.
- Use of a spermicide with a barrier device may increase the risk for a urinary tract infection in women.
- Condoms that come pre-lubricated with spermicide are not recommended. Research indicates that the spermicide does not make them any more effective than condoms without spermicide. Spermicidal lubricated condoms expire faster than those without spermicide. Non-spermicidal lubricated condoms are safe to use and are a better choice.
Condoms
The condom is the only type of birth control that protects against some sexually transmitted diseases (STDs) including HIV, the virus that causes AIDS.
Male Condom
The male condom is a thin sheath that is rolled onto an erect penis. It is about 82% effective with typical use.
Male condoms are available in different materials:
- Latex (rubber)
- Polyurethane (plastic)
- Animal membrane (usually lambskin)
Latex condoms are the most common. They are less likely to slip or break than condoms made of polyurethane. Polyurethane condoms are recommended for people who are allergic to latex or who find the smell of latex unpleasant. Condoms made from animal membrane (such as lambskin) can prevent pregnancy, but they are permeable and do not protect against sexually transmitted infections.
Most condoms come pre-lubricated. Lubricants can also be purchased and applied separately:
- Only water-based lubricants (K-Y Jelly, Astroglide, AquaLube, glycerin) should be used with latex condoms.
- Do not use petroleum jelly or other oil-based lubricant products as they can damage the condom.
- It is best to use a pre-lubricated condom or to apply a water-based lubricant. Unlubricated condoms may injure vaginal tissue and make it vulnerable to infections. Unlubricated condoms are also more likely to break.
Female Condom
The female condom is a thin 7-inch lubricated pouch made of polyurethane. It comes with a ring at both ends:
- The ring at the closed end is used to insert the device into the vagina and hold it in place over the cervix.
- The ring at the open end remains outside the vagina and partly covers the labia (lips).
The female condom offers effective protection against pregnancy and STIs. It can be inserted up to 8 hours before sex, but is visible outside of the vagina. Some women have difficulty with the insertion. Female condoms are more expensive than male condoms and (like male condoms) can only be used once.
Diaphragm
The diaphragm is a small dome-shaped latex cup with a flexible ring that fits over the cervix. The cup acts as a physical barrier against the entry of sperm into the uterus. A diaphragm is usually used along with a spermicide.
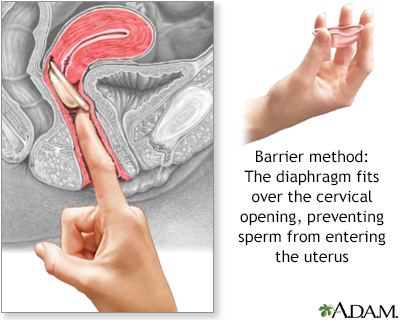
The diaphragm is a flexible rubber cup that is filled with spermicide and self-inserted over the cervix prior to intercourse. The device is left in place several hours after intercourse.
Diaphragms come in different sizes and require a prescription and fitting by a health care provider. Some women will need to be refitted with a different-sized diaphragm after pregnancy, abdominal or pelvic surgery, or weight loss or gain of 10 pounds or more. As a general rule, diaphragms should be replaced every 1 to 2 years.
Using the Diaphragm
The diaphragm can be placed in the vagina up to 1 hour before intercourse:
- Before or after each use, hold the diaphragm up to the light and fill it with water to check for holes, tears, or leaks.
- Place a small amount of spermicide (about 1 tablespoon) inside the cup, and smear some around the lip of the cup.
- Fold the diaphragm in half and insert it into the vagina by hand or with the assistance of a plastic inserter. Feel to make sure it covers the cervix.
- If you have intercourse again or more than 6 hours after inserting the diaphragm, insert some more spermicide using an applicator.
- The diaphragm must remain in the vagina for at least 6 hours after the final act of intercourse. It should not stay in place for more than 24 hours and should not be used during menstrual periods.
- The diaphragm should be washed with soap and warm water after each use and then dried and stored in its container.
Advantages of the Diaphragm
The diaphragm can be inserted up to an hour before intercourse begins, and usually (although not always) cannot be felt by either partner. It does not interfere with a woman's hormones.
Disadvantages of the Diaphragm
Some disadvantages are:
- The diaphragm is about 85% effective with typical use.
- The diaphragm can be dislodged during sex.
- The spermicide used on the diaphragm may cause irritation to the vaginal lining, which increases the risk of STIs.
- Frequent urinary tract infections and vaginal infections are a problem for some women. Be sure to urinate before inserting the device and after intercourse.
- Women who have a history of recurrent urinary tract infections, toxic shock syndrome, or allergies to latex should not use the diaphragm.
Cervical Cap
The cervical cap (FemCap) is a thimble-shaped latex cup that fits over the cervix. It is always used with a spermicidal cream or gel. It is similar to a diaphragm, but smaller, and is available in only 3 sizes (small, medium, large). The cap requires a prescription, pelvic examination, and fitting by a provider.
After a small amount of spermicide is placed in the cap, the device is inserted by hand. As in diaphragm use, instruction and practice is required. Caps wear out and should be replaced every 1 to 2 years. A refitting may also be needed when a woman experiences certain changes in her health or physical status.

Click on the icon to see an image of a cervical cap.
The cervical cap is similar to the diaphragm in terms of most advantages and disadvantages. The cap must stay in place for at least 6 hours, and not be left in place for more than 48 hours.
Rates of effectiveness depend on whether or not a woman has had children:
- For women who have never been pregnant or given birth vaginally, the cap is about 86% effective with typical use.
- For women who have given birth vaginally, the cap is about only 71% effective with typical use.
The Sponge
The sponge is a disposable form of barrier contraception. It is made of soft polyurethane foam coated with spermicide, is round in shape, and fits over the cervix like a diaphragm, but is smaller and easily portable. The Today sponge is the only brand of contraceptive sponge available in the United States.
To use the sponge, first wet it with water, and then insert it into the vagina with a finger, using the nylon cord loop attachment. The sponge can be inserted up to 24 hours before intercourse and should be left in place for at least 6 hours following intercourse. It should not be left in for more than 30 hours.
The sponge should not be used during menstruation. It should not be used soon after childbirth, miscarriage, or termination of pregnancy. Women who have had toxic shock syndrome should not use the sponge.
The sponge contains the spermicide nonoxynol-9, which may increase the risk for vaginal irritation and transmission of HIV.
For women who have never given birth, the sponge is about 88% effective with typical use. For women who have given birth, it is only about 76% effective.
Fertility Awareness Methods
Fertility awareness methods, also called natural family planning, are cycle-based methods that rely on tracking the changes in the body that signal fertility. A woman is only fertile during part of her menstrual cycle. By monitoring certain changes in her body, a woman can more or less predict the fertile phase and abstain from sexual intercourse during that time. She can also use barrier methods if they are not prohibited by religious beliefs.
Fertility awareness methods include:
- Temperature
- Cervical mucus (ovulation)
- Calendar
- Symptothermal
Temperature Method
To determine the most likely time of ovulation and therefore the time of fertility, a woman takes her
basal body temperature.
This is the body's temperature as it rises and falls in accord with hormonal fluctuations:- Each morning before rising, take your temperature with a special basal body thermometer and mark the result on a graph-paper chart.
- Note the days of menstruation and sexual activity.
- The "fertile window" is 6 days long. It starts 5 days before ovulation and ends the day of ovulation.
- The chances for fertility are considered highest between days 10 to 17 in the menstrual cycle (with day 1 being the first day of the period and ovulation occurring about 2 weeks later). However, not all women are fertile within that period of time. Women who have a longer or shorter menstrual cycle may have different time periods of fertility.
- Immediately after ovulation, the body temperature increases sharply in most cases. Some women can be ovulating normally yet not show this temperature pattern.
- By studying the temperature patterns over a few months, you can begin to anticipate ovulation and plan sexual activity accordingly.
Cervical Mucus Method
In the cervical mucus method (also called the ovulation method) you take a sample (by hand) of your cervical mucus every day for a least a month and record its quantity, appearance, and feel. You also keep track of other physical signs connected with your menstrual cycle. Cervical mucus changes in predictable ways over the course of each cycle:
- Six days before ovulation, mucus is affected by estrogen and becomes clear and elastic. Ovulation is likely to occur the last day that mucus has these properties.
- Right after ovulation, mucus is affected by progesterone and is thick, sticky, and opaque.
Calendar Method
The calendar (rhythm method) is considered the least reliable of fertility awareness methods. Women who have very irregular periods may have even less success with this method.
In the calendar method, you need to record your menstrual periods for about 6 to 12 months. You then subtract 18 days from the shortest and 11 days from the longest of the previous menstrual cycles. For example, if a woman's shortest cycle was 26 days and her longest cycle was 30 days, she must abstain from intercourse from day 8 through day 19 of each cycle.
Symptothermal Method
This method combines the temperature, cervical mucus, and calendar methods and is considered the most effective fertility awareness method. In addition, the woman tracks symptoms that may identify her fertile period. These symptoms include changes in the shape of the cervix, breast tenderness, and cramping pain.
Who Should Consider Fertility Awareness Methods?
Because of the high risk for pregnancy, fertility awareness methods are recommended only for those whose strong religious beliefs prohibit standard contraceptive methods. Couples who are not guided by religious authority, but who simply want a more natural sexual life, may use a barrier contraceptive during the fertile phase and no contraception during the rest of the cycle. However, they should understand the risk of pregnancy will be higher with this method.
To be effective against pregnancy, cycle-based methods require not only training, commitment, discipline, and perseverance, but also the cooperation of the male partner. Cycle-based methods are not recommended for women unless they are in a stable, monogamous relationship, and can count on their partner's willing participation.
Emergency Contraception
Emergency contraception is available to prevent pregnancy in situations such as:
- After sexual assault.
- After consensual intercourse in which contraception is not used.
- When contraception is used but fails (for instance, when a condom breaks or a diaphragm dislodges).
Emergency contraception is administered as a pill or, less commonly, as an IUD. Emergency contraception should not be used as a substitute for regular routine contraception. You should use emergency contraception as soon as possible after unprotected sex.
Basics of Emergency Contraception
Emergency contraception most likely works by preventing or delaying the release of an egg from a woman's ovaries. This method prevents pregnancy in the same way as birth control pills.
Types of Emergency Contraception
The emergency contraceptive pill is also known as the "morning-after" pill. There are two types of emergency contraceptive pills:
- Levonorgestrel (Plan B One-Step, Next Choice One Dose, Take Action, others)
- Ulipristal (ella)
Levonorgestrel
Levonorgestrel is a progestin that is used in many birth control pills. The levonorgestrel emergency contraceptive pill comes as a single tablet that contains 1.5 mg of levonorgestrel.
This type of emergency contraception is usually available in a drugstore aisle. Anyone can buy it without a prescription or ID.
The pill may be taken up to 3 days after unprotected intercourse.
Ulipristal
Ulipristal acetate (ella) is a newer type of emergency contraception pill that comes as a single tablet. It may be taken up to 5 days after unprotected sex.
Ulipristal requires a prescription from a health care provider. It is also available at certain health centers and family planning clinics.
Ulipristal can make birth control pills less effective. To help prevent pregnancy, you will need to use a barrier form of birth control (condom, diaphragm, spermicide) for a short time after using ulipristal.
Other Emergency Contraceptive Methods
Two other methods that may be used to prevent pregnancy after unprotected sex are:
- Birth control pills. Talk to your provider about the correct dosage. In general, you must take 2 to 5 birth control pills at the same time to have the same protection.
- A copper-releasing intrauterine device (Paragard IUD) may be used as an alternative emergency contraception method. It must be inserted by your provider within 5 days of having unprotected sex. Your provider can remove it after your next period, or you may choose to leave it in place to provide ongoing birth control.
More About Emergency Contraceptive Pills
Emergency contraception may cause side effects. Most are mild. They may include:
- Changes in menstrual bleeding
- Fatigue
- Headache and dizziness
- Nausea and vomiting
After you use emergency contraception, your next menstrual cycle may start earlier or later than usual. Your menstrual flow may be lighter or heavier than usual:
- Most women get their next period within 7 days of the expected date.
- If you do not get your period within 3 weeks after taking emergency contraception, you might be pregnant. Contact your provider.
- If you experience severe abdominal pain, be sure to contact your doctor. This may be a sign of ectopic pregnancy, which is a medical emergency.
Sometimes, emergency contraception does not work. However, research suggests that emergency contraceptives have no long-term effects on the pregnancy or a developing baby.
Other Important Facts
You should not use emergency contraception if:
- You think you have been pregnant for several days
- You have vaginal bleeding for an unknown reason (talk to your provider first)
You may be able to use emergency contraception even if you cannot regularly take birth control pills. Talk to your provider about your options.
The FDA is reviewing whether levonorgestrel emergency contraception is less likely to work in women who are above a certain weight. Some research suggests that ulipristal or the copper-releasing IUD may be more effective options for women who are overweight or obese.
Emergency contraception should not be used as a routine birth control method. It is less effective at preventing pregnancies than most types of birth control.
Female Sterilization
Female sterilization (also called tubal sterilization) is a permanent method of contraception. It offers lifelong protection against pregnancy.
Basics of Female Sterilization
Female sterilization procedures block the fallopian tubes and thereby prevent sperm from reaching and fertilizing the eggs. The ovaries continue to function normally, but the eggs they release break up and are harmlessly absorbed by the body.
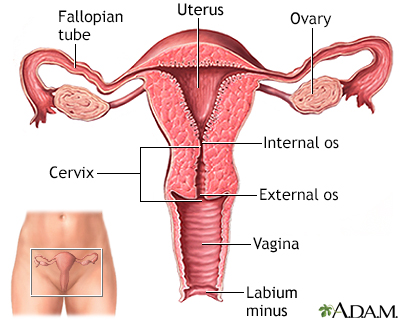
The female reproductive system includes the vagina, cervix, uterus, ovaries, and fallopian tubes. When an egg is released by an ovary, it travels to the fallopian tube to await fertilization. If fertilization occurs, the egg moves to the uterus and implants in the uterine lining. If no fertilization occurs, the egg moves to the uterus and disintegrates.
Sterilization does not cause menopause. Menstruation continues as before, with usually very little difference in length, regularity, flow, or cramping. Sterilization does not offer protection against sexually transmitted infections. Women still need to use a condom for protection.

Click on the icon to see an image of tubal ligation.
Surgical Methods (Tubal Ligation)
Tubal ligation, also called tube tying, is the surgical method for female sterilization. It is performed in a hospital or outpatient clinic under local or general anesthesia. There are two main approaches, laparoscopy and minilaparotomy ("mini-lap"):
Laparoscopy
is the most common approach. The abdomen is inflated with gas to allow better view of the organs. The surgeon makes a tiny incision near the navel and inserts a narrow tube with a camera on the end (laparoscope). Surgical instruments are inserted through the laparoscope or a separate incision.Minilaparotomy
is usually performed after childbirth. No gas or laparoscope is used. A small incision is made near the pubic hairline.
The surgeon locates the fallopian tubes and closes them using different methods. The tubes may be cut and tied into a knot, burned shut (cauterization) or clamped off with a small clip or ring.
The procedure takes about 20 to 30 minutes and causes minimal scarring. You can usually go home the same day. You can return to most normal activities within a few days, but should avoid heavy lifting for 3 weeks.

Click on the icon to see an illustrated series detailing tubal ligation.
Considerations Before Female Sterilization
Before undergoing sterilization, a woman must be sure that she will not want to bear children in the future, even if the circumstances of her life change. She must also be aware of the many effective contraceptive choices available. Possible reasons for choosing female sterilization procedures over reversible forms of contraception include:
- Not wanting children and being unable to use other methods of contraception
- Health problems that make pregnancy unsafe
- Genetic disorders
If in a relationship, both partners should completely agree that they no longer want to have children. They should also have ruled out vasectomy for the man. Vasectomy is a simple procedure that has a lower failure rate than female surgical sterilization, carries fewer risks, and is less expensive.
If a woman changes her mind and wants to become pregnant, a reversal procedure is available, but it is very difficult to perform and requires an experienced surgeon. Subsequent pregnancy rates after reversal depend on the surgeon's skill, the age of the woman, and, to a lesser degree, her weight and the length of time between the tubal ligation and the reversal procedure. Not all insurance carriers cover the cost of reversal.
Advantages of Female Sterilization
Women who choose sterilization no longer need to worry about pregnancy or cope with the distractions and possible side effects of contraceptives. Sterilization does not impair sexual desire or pleasure. Some people find it enhances sex by removing the fear of unwanted pregnancy.
Disadvantages of Female Sterilization
- Incomplete closing of the tubes, which could make pregnancy still possible. About 1 in 200 women who have had tubal ligation get pregnant later.
- Increased risk of a tubal (ectopic) pregnancy if pregnancy occurs after a tubal ligation.
- After laparoscopy, a woman may feel dizzy, nauseous, bloated, or gassy, and may have minor abdominal and shoulder pain. Usually these symptoms go away in 1 to 3 days.
Serious complications from female surgical sterilization are uncommon but may include bleeding, infection, or injury to nearby organs or tissues from surgical instruments.
Resources
- National Institute of Child Health and Human Development -- www.nichd.nih.gov
- Planned Parenthood -- www.plannedparenthood.org
- American College of Obstetricians and Gynecologists -- www.acog.org
- Association of Reproductive Health Professionals -- www.arhp.org
References
American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 206: Use of hormonal contraception in women with coexisting medical conditions. Obstet Gynecol. 2019;133(2):396-399. PMID : 30681537 www.ncbi.nlm.nih.gov/pubmed/30681537.
American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 112: Emergency contraception. Obstet Gynecol. 2010;115(5):1100-1109. PMID: 20410799 www.ncbi.nlm.nih.gov/pubmed/20410799.
American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 121: Long-acting reversible contraception: Implants and intrauterine devices. Obstet Gynecol. 2011;118(1):184-196. PMID: 21691183 www.ncbi.nlm.nih.gov/pubmed/21691183.
Committee on Adolescent Health Care. Committee Opinion No 699: Adolescent pregnancy, contraception, and sexual activity. Obstet Gynecol. 2017;129(5):e142-e149. PMID: 28426620 www.ncbi.nlm.nih.gov/pubmed/28426620.
Curtis KM, Jatlaoui TC, Tepper NK, et al. U.S. selected practice recommendations for contraceptive use, 2016. MMWR Recomm Rep. 2016;65(4):1-66. PMID: 27467319 www.ncbi.nlm.nih.gov/pubmed/27467319.
Curtis KM, Tepper NK, Jatlaoui TC, et al. U.S. medical eligibility criteria for contraceptive use, 2016. MMWR Recomm Rep. 2016;65(3):1-103. PMID: 27467196 www.ncbi.nlm.nih.gov/pubmed/27467196.
Curtis KM, Peipert JF. Long-acting reversible contraception. N Engl J Med. 2017;376(5):461-468. PMID: 28146650 www.ncbi.nlm.nih.gov/pubmed/28146650.
Gallo MF, Legardy-Williams J, Hylton-Kong T, et al. Association of progestin contraceptive implant and weight gain. Obstet Gynecol. 2016;127(3):573-576. PMID: 26855107 www.ncbi.nlm.nih.gov/pubmed/26855107.
Gavin L, Moskosky S, Carter M, et al. Providing quality family planning services: Recommendations of CDC and the U.S. Office of Population Affairs. MMWR Recomm Rep. 2014;63(RR-04):1-54. PMID 24759690 www.ncbi.nlm.nih.gov/pubmed/24759690.
Glasier A. Contraception. In: Jameson JL, De Groot LJ, de Kretser DM, et al, eds. Endocrinology: Adult and Pediatric. 7th ed. Philadelphia, PA: Elsevier Saunders; 2016:chap 134.
Isley MM, Katz VL. Postpartum care and long-term health considerations. In: Gabbe SG, Niebyl JR, Simpson JL, et al, eds. Obstetrics: Normal and Problem Pregnancies. 7th ed. Philadelphia, PA: Elsevier; 2017:chap 23.
Jatlaoui TC, Ermias Y, Zapata LB. Contraception. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 143.
Lopez LM, Bernholc A, Chen M, et al. Hormonal contraceptives for contraception in overweight or obese women. Cochrane Database Syst Rev. 2016;(8):CD008452. PMID: 27537097 www.ncbi.nlm.nih.gov/pubmed/27537097.
Lopez LM, Grimes DA, Gallo MF, Stockton LL, Schulz KF. Skin patch and vaginal ring versus combined oral contraceptives for contraception. Cochrane Database Syst Rev. 2013;(4):CD003552. PMID: 23633314 www.ncbi.nlm.nih.gov/pubmed/23633314.
Ott MA, Sucato GS; Committee on Adolescence. Contraception for adolescents. Pediatrics. 2014;134(4):e1257-e1281. PMID 25266435 www.ncbi.nlm.nih.gov/pubmed/25266435.
Secura GM, Madden T, McNicholas C, et al. Provision of no-cost, long-acting contraception and teenage pregnancy. N Engl J Med. 2014;371(14):1316-1323. PMID 25271604 www.ncbi.nlm.nih.gov/pubmed/25271604.
Tepper NK, Krashin JW, Curtis KM, Cox S, Whiteman MK. Update to CDC's U.S. medical eligibility criteria for contraceptive use, 2016: Revised recommendations for the use of hormonal contraception among women at high risk for HIV infection. MMWR Morb Mortal Wkly Rep. 2017;66(37):990-994. PMID: 28934178 www.ncbi.nlm.nih.gov/pubmed/28934178.
|
Review Date:
7/20/2019 Reviewed By: John D. Jacobson, MD, Professor of Obstetrics and Gynecology, Loma Linda University School of Medicine, Loma Linda Center for Fertility, Loma Linda, CA. Also reviewed by David Zieve, MD, MHA, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. |
 All rights reserved.
All rights reserved.