

Carpal tunnel syndrome - InDepth
Highlights
Overview
- Carpal tunnel syndrome (CTS) is a disorder that causes pain and weakness in the hand and wrist.
- In general, carpal tunnel syndrome develops when the tissues around the median nerve of the hand swell and press on the nerve.
- Some research suggests that this swelling is caused by a buildup of fluid (called synovial fluid) under the lining.
- Anyone with recurrent or persistent pain, numbness and tingling, or weakness of the hand and wrist should consult a doctor for an evaluation.
- Early in the disorder, the process is reversible. Over time, however, permanent nerve damage may develop.
- It is often very difficult to determine the precise cause of carpal tunnel syndrome
Risk Factors
- Although some studies have suggested that over half of CTS cases are associated with workplace factors, most studies now indicate that CTS is primarily associated with medical or physical conditions such as diabetes, osteoarthritis, hypothyroidism, acromegaly, sarcoidosis, pregnancy, and rheumatoid arthritis.
- Women have a significantly higher risk for carpal tunnel syndrome than men.
- Older, overweight, and physically inactive people are at higher risk.
Treatment
- It is important to begin treating early carpal tunnel syndrome before the damage progresses.
- A conservative approach to CTS, which may include corticosteroid injections and bracing, is the first step in treating this disorder.
- Surgery is usually an effective treatment choice for people with the more advanced signs and symptoms of carpal tunnel syndrome who do not recover after conservative treatment.
Introduction
Carpal tunnel syndrome (CTS) is a disorder that causes pain and weakness in the hand and wrist. CTS develops from problems in a nerve in the wrist -- not the muscles, as some people believe. The symptoms of CTS can range from mild to incapacitating.
The Carpal Tunnel and Median Nerve
To understand how CTS arises, it is important to know the parts of the hand and wrist that are involved.
The Carpal Tunnel
The carpal tunnel is a passageway that forms beneath the strong, broad
transverse ligament
. This ligament is a bridge that extends across the lower palm and connects the bones of the wrist (carpus or carpal bones
) that form an arch above the tunnel.The Median Nerve and Flexor Tendons
The
median nerve
and nineflexor tendons
pass under the ligament bridge and through the carpal tunnel (similar to a river under a bridge). They extend from the forearm up into the hand:- The flexor tendons are fibrous cords that connect the muscles in the forearm to the fingers (two to each finger and one to the thumb.) They allow flexing of the fingers and clenching of the fist.
- The median nerve plays two important roles. It supplies sensation to the palm side of the thumb, index, middle, and ring fingers, and to the flexor tendons. It provides function for the muscles at the base of the thumb (the thenar muscles).
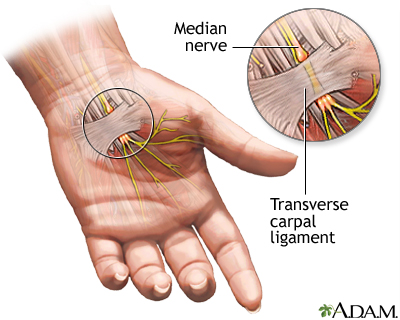
The median nerve travels through a compartment in the wrist called the carpal tunnel. The ligaments that traverse the tunnel are not very flexible. Any swelling within the wrist compartment can put excessive pressure on structures such as the blood vessels and the median nerve. Excessive pressure can constrict blood flow and cause nerve damage. The symptoms from the compression cause pain, loss of sensation, and decreased function in the hand.
The Carpal Tunnel Syndrome Process
It is not completely known how the process leading to CTS actually evolves, and how nerve conduction (the transmission of the nerve signal) through the wrist changes. In general, CTS develops when the tissues around the median nerve swell and press on the nerve. Early in the disorder, the process is reversible. Over time, however, the insulation on the nerves may wear away, and permanent nerve damage may develop.
The following events have been observed in the hands of people with carpal tunnel syndrome:
- The protective lining of tendons (called the
tenosynovium
) swells within the carpal tunnel. Some research suggests that this swelling is caused by a buildup of fluid (called synovial fluid) under the lining.Synovial fluid
normally lubricates and protects the tendons. - The
transverse ligament
, the band of fibrous tissue that forms the roof over the median nerve, becomes thicker and broader. - The swollen tendons and thickened ligament press on the median nerve fibers, just as stepping on a hose slows the flow of water through it. This compression reduces blood flow and oxygen supply to the nerve, while slowing the transmission of nerve signals through the carpal tunnel. Some cases of CTS may be due to enlargement of the median nerve rather than compression by surrounding tissues.
The result of these processes is pain, numbness, and tingling in the wrist, hand, and fingers. Only the little finger is unaffected by the median nerve.

Click the icon to see an image of carpal tunnel syndrome.
Symptoms
Symptoms of CTS usually progress gradually over weeks and months, or sometimes years. Anyone with recurrent or persistent pain, numbness and tingling, or weakness of the hand, especially on the thumb and index side of the hand should consult a doctor for a diagnosis. Symptoms often develop as follows:
- Initial symptoms include pain in the wrist and palm side of the hand. Problems commonly occur in both hands. (Even when only one hand is painful, the other hand often shows signs of nerve conduction abnormalities when tested.)
- Early on, the patient also usually reports numbness, tingling, burning, or some combination of symptoms on the palm side of the index, middle, and ring fingers. (Typically the fifth finger has no symptoms.) Such sensations may radiate to the forearm or shoulder.
- Over time, the hand may become numb, and patients may lose the ability to feel heat and cold. Patients may experience a sense of weakness and a tendency to drop things.
- Patients may feel that their hands are swollen even though there is no visible swelling. This symptom may actually prove to be an important indicator of greater CTS severity.
Symptoms may occur not only when the hand is being used but also at night when the patient is at rest. Even in cases where work is the suspected cause, symptoms typically first occur outside of work. In fact, the disorder may be distinguished from similar conditions by pain that occurs at night after going to bed.
Causes
Biological Causes
CTS is considered an inflammatory disorder caused by repetitive stress, physical injury, or a medical condition. It is often very difficult, however, to determine the precise cause of carpal tunnel syndrome. No tests are available to identify a specific cause. Except in patients with certain underlying diseases, the biological mechanisms leading to CTS are unknown.
Working Conditions versus Medical Problems
Although some studies suggest that more than half of CTS cases are associated with workplace factors, there is no strong evidence of a cause-and-effect relationship. In fact, most studies now strongly suggest that CTS is primarily associated with medical or physical conditions such as diabetes, osteoarthritis, hypothyroidism, and rheumatoid arthritis.
CTS also tends to occur in people with certain genetic or environmental risk factors. These risk factors include obesity, smoking, alcohol abuse, or significant mental stress. CTS sometimes runs in families, which suggests that it has some type of genetic origin. When people who are susceptible to CTS are subjected to repetitive hand or wrist work, the risk for CTS can become significant. CTS, then, is very likely to be due to a combination of factors that lead to nerve damage in the hand.
Work-Related Issues and Carpal Tunnel Syndrome
High Force and Vibration
Even though medical and physical conditions may be the initial culprits leading to CTS, certain working conditions may be linked to nerve damage. Work that involves high force or vibration is particularly hazardous, as is repetitive hand and wrist work in cold temperatures.
In addition to CTS, other disorders of the hand and wrist result from these work-related movements. They include the following:
- Hand-arm vibration syndrome. Tingling and numbness that persist even after the vibration stops.
- Cumulative trauma (repetitive stress) disorder
- Overuse syndromes
- Chronic upper limb pain syndrome
All of these problems are generally associated with repetitive and forceful use of the hands, resulting in damaged muscles and bones of the upper arms.
Medical Conditions
Several medical conditions increase the risk for, or even cause CTS. The main conditions associated with CTS are diabetes, hypothyroidism, rheumatoid arthritis, osteoarthritis, acromegaly, sarcoidosis, amyloid infiltration of the transverse carpal ligament, obesity, and pregnancy. Many of the underlying diseases that contribute to the development of CTS are also associated with more severe forms of CTS.
Diabetes
CTS is a very common feature of diabetic neuropathy, one of the major complications of diabetes. Neuropathy is decreased or distorted nerve function; it particularly affects sensation. Symptoms include numbness, tingling, weakness, and burning sensations, usually starting in the fingers and toes and moving up to the arms and legs. About 14% to 30% of patients with CTS have diabetes. Both type 1 and type 2 diabetes increase the risk for CTS. The development of CTS symptoms is related to the patient's age, and the length of time that he or she has had diabetes.
Autoimmune Diseases
In autoimmune diseases, the body's immune system abnormally attacks its own tissue, causing widespread inflammation, which, in many cases, affects the carpal tunnel of the hand. Such autoimmune diseases include rheumatoid arthritis, systemic lupus erythematosus, and thyroiditis, which can lead to hypothyroidism. Some experts believe that CTS may actually be one of the first symptoms in a number of these diseases. Studies also suggest that CTS patients with these disorders are more likely to have severe CTS that requires surgery.
Diseases that Affect Muscle and Bones
Arthritis, gout, and other medical conditions that damage the muscles, joints, or bones in the hand may cause changes that lead to CTS.
Structural Abnormalities
Inborn abnormalities in the bones of the hand, wrist, or forearm may contribute to CTS.
Chronic Kidney Disease
People with chronic kidney disease who are on hemodialysis for a long time often experience beta 2-microglobulin amyloidosis. This condition arises from buildup of a certain type of protein, called beta 2-microglobulin, in different organs, including the joints of the hand. This buildup can result in CTS. The longer the person has been receiving hemodialysis, the greater the risk of CTS. Certain drugs and procedures (particularly a procedure called hemodiafiltration) may be able to reduce microglobulin build-up.
Other Diseases
Other medical conditions may cause or increase susceptibility to CTS:
- Down syndrome
- Amyloidosis (a progressive disorder of the connective tissues that lead to accumulation of a substance called amyloid)
- Acromegaly (a disease that leads to abnormally large hands and feet due to excessive growth hormone)
- Tumor on the median nerve (removing the tumor often successfully treats CTS in these cases)
Medications
According to case reports, many medications may increase the risk for temporary CTS. They include certain medications that affect the immune system (such as interleukin-2) and anticlotting drugs (such as warfarin). The evidence is conflicting as to whether corticosteroids and hormone replacement therapy may increase the risk of CTS. More research is needed before a cause-and-effect relationship can be established.
Injuries
Bone dislocations and fractures can cause swelling or narrowing of the carpal tunnel and put pressure on the median nerve.
Hormonal Changes
Hormonal fluctuations in women play a role in CTS. Such fluctuations may lead to fluid retention and other changes that cause swelling in the body. Fluid retention is one reason that CTS may develop during pregnancy.
Genetic Factors
CTS is associated with a family history of the disorder. Certain physical characteristics or medical conditions that are associated with CTS also run in families. CTS in young people most likely has a genetic component.
Other genetic factors that may contribute to this disorder include abnormalities in certain genes that regulate myelin, a fatty substance that insulates nerve fibers.
Risk Factors
Evidence suggests that about 3% of women and 2% of men will be diagnosed with CTS during their lifetime. The condition peaks in women over age 55. Still, determining how many people actually have CTS is very difficult. Many people who report CTS symptoms have normal test results. Other people have abnormal test results but no symptoms.
Age
Older people are at higher risk for CTS than younger adults. CTS is very rare in children.
Women
Some studies indicate that women may have a higher risk for CTS than men. The explanation for this greater risk is unknown, but it may be related to the smaller size of a woman's carpal tunnel. Hormonal changes also appear to play a major role in CTS.
In pregnant women, CTS may occur in both wrists. CTS that begins during pregnancy is usually not severe and persistent enough to require treatment. Although cases eventually go away on their own after delivery, symptoms may persist for 6 months or more.
CTS has also been shown to increase:
- After delivering a baby
- During menopause
Women are also at a much higher risk for autoimmune disorders than men. These disorders are significantly linked to CTS.
Obesity and Lack of Fitness
Being overweight is a consistent risk factor for CTS. Greater body mass appears to reduce the speed of nerve messages into the hand. Obesity is also related to poor physical fitness, which may increase risk. Weight is strongly linked to CTS in patients under age 63, but it may be a less important factor as people get older.
Specific Workers at Risk for CTS
Workers who use their hands and wrists repetitively are at risk for CTS, particularly if they work in cold temperatures and have factors or medical conditions that make them susceptible to the condition.
Computer Users and Typists
Repetitive typing and key entry has traditionally been associated with missing work due to CTS. The risk for CTS in this group, however, is still much lower than it is in occupations involving heavy labor. Although more than 10% of computer users complain of CTS symptoms, the evidence implicating computer use as a major cause of CTS is weak.
Other Very High-Risk Workers
Workers in the meat and fish packing industries and those who assemble airplanes have the highest risk for CTS, according to one study. Meat packers complained of pain and loss of hand function as long ago as the 1860s. Even today, the incidence of CTS in the meat, poultry, and fish packing industries may be as high as 15%. CTS may also affect as many as 10% of automobile workers. Any types of assembly work may also raise the risk for CTS.
CTS is also more frequent in people whose work involves hand-held vibratory tools, such as rock drills and chainsaws, including quarry frilling and forestry workers.
Musicians
Musicians are at very high risk for CTS and other problems related to the muscles and nerves in the hands, upper trunk, and neck. In one study, 20% of musicians reported CTS or other nerve disorders in the hands and wrists.
Psychosocial Factors in the Workplace
Studies indicate that psychosocial factors in the workplace, such as intense deadlines, a poor social work environment, and low levels of job satisfaction are major contributors to carpal tunnel pain.
At Home and Play
People who intensively cook, knit, sew, do needlepoint, play computer games, do carpentry, or use power tools are at increased risk for CTS. Long-distance cycling may worsen symptoms of carpal tunnel syndrome.
Other Physical Characteristics
Square Wrists
Some (but not all) studies have reported a higher risk for CTS in people with square wrists (the thickness and width are about the same) than in those with the more common rectangular wrists.
Palm Shape
In one study, patients with palms that were both shorter and wider than average, and who also had shorter third fingers, were more likely to have CTS than those without these hand characteristics.
Smoking and Alcohol Abuse
Cigarette smoking slows blood flow, which is why smokers have more severe symptoms and slower recovery than nonsmokers. Increased alcohol intake has been associated with CTS in people who also have other risk factors.
Other Factors
Poor nutrition, previous injuries, and stress can increase the risk for carpal tunnel syndrome. In addition, high levels of so-called "bad" cholesterol (low-density lipoprotein, or LDL) have been linked to an increased risk of CTS.
Prognosis
Carpal tunnel syndrome can range from a minor inconvenience to a disabling condition, depending on its cause and persistence, and the patient's individual characteristics. Many cases of CTS are mild, and when symptoms don't last long, they often get better on their own. Once a woman with pregnancy-associated CTS gives birth, for instance, the swelling in her wrists and other symptoms almost always subside. Proper treatment of the medical conditions that cause CTS can often help reduce wrist swelling.
In severe untreated cases, however, the muscles at the base of the thumb may wither, and loss of sensation may be permanent. CTS can become so crippling that people can no longer do their jobs or even perform simple tasks at home.
Impact on Work and Livelihood
According to a report from the Bureau of Labor Statistics, carpal tunnel syndrome was associated with the second longest average time away from work (28 days) among the major disabling diseases and illnesses in all private industries. (Fractures were first, with an average of 31 days away.)
Eventually, workers with CTS may be forced to give up their livelihood. Because of the controversy surrounding the issue of carpal tunnel syndrome and workers' compensation, workers may not always receive compensation payments.
Prevention
Because many factors can contribute to CTS, there is no single way to prevent it. Treating any underlying medical condition is important. Simple common sense may help minimize some of the risk factors that predispose a person to work-related CTS or other cumulative trauma disorders. A patient can learn how to adjust the work area, handle tools, or perform tasks in ways that put less stress on the hands and wrists. Proper posture and exercise programs to strengthen the fingers, hands, wrists, forearms, shoulders, and neck may help prevent CTS.
Corporate Efforts
Many companies are now taking action to help prevent repetitive stress injuries. These efforts include modifying equipment, tasks, and processes. Changes in workstations and jobs, as well as buying new equipment may be tried. It should be stressed, however, that there has been no evidence that any of these methods can provide complete protection against CTS. The optimal corporate approach, if possible, is to reallocate workers with repetitive stress injuries to other jobs.
Preventing CTS in Keyboard Workers
Altering the way a person performs repetitive activities and replacing old tools with ergonomically designed new ones may help prevent inflammation in the hand and wrist. Most of the interventions described below have been found to reduce repetitive motion problems in the muscles and tendons of the hand and arm. They may reduce the incidence of carpal tunnel syndrome, although there is no definite proof of this effect.
Rest Periods and Avoiding Repetition
Anyone who does repetitive tasks should begin with a short warm-up period, take frequent breaks, and avoid overexertion of the hand and finger muscles whenever possible. Employers should be urged to vary their employees' tasks and work.
Taking multiple "microbreaks" (about 3 minutes each) reduces strain and discomfort without decreasing productivity. Such breaks may include the following:
- Shaking or stretching the limbs
- Leaning back in the chair
- Squeezing the shoulder blades together
- Taking deep breaths
Good Posture
Good posture is extremely important in preventing carpal tunnel syndrome, particularly for typists and computer users.
- The worker should sit with the spine against the back of the chair with the shoulders relaxed.
- The elbows should rest along the sides of the body, with wrists straight.
- The feet should be firmly on the floor or on a footrest.
- Typing materials should be at eye level so that the neck does not bend over the work.
- Keeping the neck flexible and the head upright maintains circulation and nerve function to the arms and hands. One method for finding the correct head position is the "pigeon" movement. Keeping the chin level, glide the head slowly and gently forward and backward in small movements, avoiding neck discomfort.
Good Office Furniture
Poorly designed office furniture is a major contributor to bad posture. Chairs should be adjustable for height, with a supportive backrest. Custom-designed chairs, made for people who do not fit in standard chairs, can be expensive. However, these costs can save companies on the medical expenses that follow injuries related to bad posture.
Voice Recognition Software
For CTS patients who must use a computer frequently, voice recognition software (Dragon NaturallySpeaking, MacSpeech) may allow virtually hands-free computer use.
Keyboard and Mouse Tips
Anyone who uses a keyboard and mouse has options that may help protect the hands.
- Adjust the tension of the keys so they can be depressed without excessive force.
- Keep the hands and wrists in a relaxed position to avoid excessive force on the keyboard.
- Replace the mouse with a trackball device and the standard keyboard with a jointed-type keyboard.
- Use wrist rests, which fit under most keyboards, to help keep the wrists and fingers in a comfortable position.
- Keep the computer mouse as close to the keyboard and the user's body as possible, to reduce shoulder muscle movement.
- Hold the mouse lightly, with the wrist and forearm relaxed. New mouse supports are also available that relieve stress on the hand and support the wrist.
- Cut mouse pads in half to reduce movement.
Innovative keyboard designs may reduce hand stress. Ergonomic keyboards allow the user to adjust and modify hand positions and key tension. Most have a split or "slanted" keyboard that places the wrists at an angle. Studies suggest these keyboards help keep the wrist in a more neutral position.
Reducing Force from Hand Tools
The force placed on the fingers, hands, and wrists by a repetitive task is an important contributor to CTS. To alleviate the effect of force on the wrist, design tools and tasks so that the wrist position is the same as it would be if the arms dangled relaxed at the sides.
- No task should require the wrist to deviate from side to side or to remain flexed or highly extended for long periods of time.
- The handles of hand tools such as screwdrivers, scrapers, paintbrushes, and buffers should be designed so that the force of the worker's grip is distributed across the muscle between the base of the thumb and the little finger, not just in the center of the palm.
- People who need to hold tools (including pencils and steering wheels) for long periods of time should grip them as loosely as possible.
- In order to apply force appropriately, the ability to feel an object is extremely important. Tools with textured handles are helpful.
- If possible, people should avoid working at low temperatures, which reduces sensation in the hands and fingers.
- Power tools and machines should be designed to minimize vibrations.
- Wearing thick gloves, when possible, may lessen the shock transmitted to the hands and wrists.
Hand and Wrist Exercises for the Prevention of Carpal Tunnel Syndrome
Hand and wrist exercises may help reduce the risk of developing carpal tunnel syndrome. Isometric and stretching exercises can strengthen the muscles in the wrists and hands, as well as in the neck and shoulders, improving blood flow to these areas. Performing the simple exercises described below for 4 to 5 minutes every hour may be helpful.
Exercises for Carpal Tunnel Syndrome | |
Wrists | Exercise 1
|
Exercise 2
| |
Exercise 3 (Wrist Circle)
| |
Fingers and Hand | Exercise 1
|
Exercise 2
| |
Exercise 3
| |
Forearms (stretching these muscles will reduce tension in the wrist) |
|
Neck and Shoulders | Exercise 1
|
Exercise 2
| |
Diagnosis
CTS is most accurately diagnosed using a medical history, the patient's descriptions of symptoms, a physical examination, and electrodiagnostic tests that measure nerve conduction through the hand.
Diagnosing CTS, however, is not straightforward. Only a small fraction of patients exhibit all three factors necessary for a clear diagnosis:
- Classic CTS symptoms
- Specific physical findings
- Abnormal electrodiagnostic test results
Many people have abnormal electrodiagnostic test results without classic symptoms or any symptoms at all. Furthermore, about 15% of the population has symptoms that are consistent with CTS, but in most of these people, test results do not indicate the disorder.
MRI, CT scans, and other imaging tests are not useful for diagnosing carpal tunnel syndrome.
Symptom Description and Severity
Many cases of CTS result from a medical problem that is worsened by repetitive stress factors at work. The patient should give the doctor a detailed history and description of any complaints, in any part of the body. The patient should report in detail any daily activities that require repetitive hand or wrist actions, abnormal postures, or other regular situations that could affect the nerves in the neck, shoulders, and hands. The patient should also report whether the symptoms are more likely to appear at night, or after particular tasks.
Questionnaires
The use of specific questionnaires that score results can accurately assess the severity of the condition.
Hand Diagram
A diagram of the hand and wrist, usually divided into six regions, is a very useful diagnostic tool. Patients are asked to indicate where their symptoms are, including pain, numbness, or tingling, by locating the affected areas on the diagram. They may also be asked to rate the severity of their symptoms. A diagnosis is probable if at least two of fingers 1, 2, or 3 have these symptoms, and if there is pain in or near the wrist. CTS is possible if at least one of these fingers has symptoms. It is unlikely if there are no symptoms in these fingers, the palm, or the wrist.
Ruling out Underlying Medical Disorders
One of the most important first steps in diagnosing CTS is to evaluate any underlying medical disorders that may be contributing to the condition. Experts emphasize the need to fully examine patients with symptoms of CTS. Relying only on CTS symptoms and personal or work histories may fail to detect (and thus properly treat) underlying medical conditions that could be serious. If the doctor suspects that an underlying medical condition may be exacerbating the symptoms of CTS, laboratory tests will be performed. Tests for thyroid disease and rheumatoid arthritis may be helpful. The doctor may take an x-ray, for example, to check for arthritis or fractured bones.
Arthritic Conditions
Arthritic conditions, including rheumatoid arthritis, gout, and osteoarthritis, can all cause pain in the hands and fingers that may mimic carpal tunnel syndrome.
Muscle and Nerve Diseases
Any disease or abnormality that affects the muscles and nerves, including those in the spine, may produce symptoms in the hand that mimic carpal tunnel syndrome.
Ruling Out Other Cumulative Trauma Disorders
About 25% of patients with suspected work-related cumulative trauma or repetitive stress disorders have evidence of other conditions that resemble, but are not carpal tunnel syndrome. A definitive diagnosis is often difficult. Most of these disorders require treatments similar to those used for CTS: rest, immobilization, steroid injections, and surgery if conservative treatment is unsuccessful.
Other Cumulative Trauma Disorders | |
Location | Description |
The Median Nerve in Other Locations | Repetitive work can cause pressure on the median nerve in locations other than the wrist and can also affect other nerves in the arm and hand. The branch of the median nerve that runs through the palm of the hand can be damaged directly by repeated pounding or by the use of certain tools that are gripped with the palm, such as needle-nosed pliers. The median nerve can also be pinched in the forearm. |
Guyon Canal Syndrome (Commonly called ulnar tunnel syndrome) | The ulnar nerve can, like the median nerve, be trapped as a result of repetitive stress. When this nerve is trapped, the condition is sometimes referred to as ulnar tunnel syndrome. It is also known as Guyon canal syndrome, because this is the name of the passage through which the ulnar nerve passes. General symptoms are similar to those of carpal tunnel syndrome, but patients experience a loss of sensation in the ring and little finger and in the outer half of the palm. Guyon canal syndrome can be a separate problem, although it commonly occurs with CTS. In such cases, release surgery for CTS usually also relieves the ulnar nerve entrapment. The ulnar nerve can also be affected at the elbow. |
De Quervain's Tenosynovitis | Tenosynovitis is swelling of the slippery covering of the tendons that move the thumb. When it causes pain on the side of the wrist and forearm right below the base of the thumb, it is known as De Quervain's tenosynovitis. (Finklestein's Test may help identify this. Make a fist that encloses the thumb, and bend the wrist sideways and down away from the thumb. If it causes pain, it is likely to be De Quervain's tenosynovitis.) It may be treated with splints or corticosteroid injections. In severe cases release surgery is effective. |
Digital Flexor Tenosynovitis (Trigger or Snapping Finger) | Digital flexor tenosynovitis, commonly called trigger or snapping finger, is brought on when a tendon thickens, leaving the finger or thumb in a bent position. This disorder usually occurs when the tendons form a knot. It may be a problem in people with hypothyroidism, diabetes, gout, rheumatoid arthritis, or connective tissue disorders. Digital flexor tenosynovitis can cause pain and a clicking sound when the trigger finger or thumb is bent and straightened. It can be effectively treated with corticosteroid injections. |
Thoracic Outlet Syndrome | Thoracic outlet syndrome is caused by the compression of nerves or blood vessels running down the neck into the arm. The compression occurs at the first rib in the front of the shoulder. This may happen after an accident or simply from repeatedly slouching. It can produce symptoms very similar to those of CTS. Other symptoms may include Raynaud's phenomenon (changes in sensation and temperature in the hand). A doctor may be able to diagnose the condition by detecting reduced blood flow in the arm as the patient raises the affected hand and turns his or her head toward the opposite side. Although the condition is uncommon, a correct diagnosis is important to differentiate it from CTS, since treatments differ. Surgery may be required to relieve pressure on the nerves and blood vessels. |
Cervical Radiculopathy | Cervical radiculopathy, or pinched nerve, in the neck can lead to the median nerve being more vulnerable around the wrist. The nerve can exhibit "double crush syndrome" where it was pinched near the neck and also again near the wrist. The nerve is more vulnerable to produce symptoms even with the compression at each site is not as severe. Neck physical therapy or nerve root injection or cervical disc surgery can elevate the symptoms. |
Physical Assessment Tests for Carpal Tunnel Syndrome
The doctor will perform a physical exam.
The following findings are helpful in identifying carpal tunnel syndrome:
- Less sensitivity to pain where the median nerve runs to the fingers
- Thumb weakness
- Inability to tell the difference between one and two sharp points on the fingertips (this is a late sign of carpal tunnel)
Flick Signal
One important and simple test of carpal tunnel is the "flick" signal:
- The patient is asked, "What do you do when your symptoms are worse?"
- If the patient responds with a motion that resembles shaking a thermometer, the doctor can strongly suspect carpal tunnel.
Testing for Thumb Weakness
Two questions are useful in determining thumb weakness:
- Can the thumb rise up from the plane of the palm?
- Can the thumb stretch so that its pad rests on the little finger pad?
Provocation Tests
Certain tests can produce symptoms:
Phalen's Test.
In Phalen's test, the patient rests the elbows on a table and lets the wrists dangle with fingers pointing down and the backs of the hands pressed together. If symptoms develop within a minute, CTS is more likely. (If the test lasts for more than a minute, even patients without CTS may develop symptoms.) This test may be particularly important in determining the severity of CTS and assessing the results of treatment.Tinel's Sign.
In the Tinel's sign test, the doctor taps over the median nerve to produce a tingling or mild shock sensation.Pressure Provocation Test.
The doctor presses over the carpal tunnel for 30 seconds to produce tingling or shock in the median nerve.Tourniquet Test.
This test uses an inflatable cuff that applies pressure over the median nerve to produce tingling or small shocks.Hand Elevation Test.
The patient raises his or her hand overhead for 2 minutes to produce symptoms of CTS. The test was has been proven to be accurate and may provide useful information when combined with the Tinel's and Phalen's tests.
Electrodiagnostic Tests
Electrodiagnostic tests analyze the electric waves of nerves and muscles. These tests can help detect median nerve compression in the carpal tunnel.
Electrodiagnostic tests should be used if clinical or provocative tests are positive and the patient is considering surgery. These tests are the best methods for confirming a diagnosis of CTS. According to the American Association of Neuromuscular and Electrodiagnostic Medicine, doctors who perform these tests should be certified by the American Board of Electrodiagnostic Medicine. Specific electrodiagnostic tests, called nerve conduction studies and electromyography, are the most common ones performed. Nerve conduction tests can also detect other problems that cause CTS symptoms, such as pinched nerves in the neck or elbow, or thoracic outlet syndrome.
Nerve Conduction Studies.
To perform nerve conduction studies, surface electrodes are first fastened to the hand and wrist. Small electric signals are then applied to the nerves in the fingers, wrist, and forearm to measure how fast a signal travels through the nerves that control movement and sensation. Nerve conduction tests are fairly accurate when done on patients with more clear-cut symptoms of carpal tunnel syndrome. They are less accurate in identifying mild CTS, however. Patients should be sure their practitioners perform tests that compare a number of internal responses, not just the responses of muscles located in the palm at the base of the thumb. They should also make sure the tests measure responses on the second or third fingers.Electromyography.
To perform electromyography, a thin, sterile wire electrode is inserted briefly into a muscle, and the electrical activity is displayed on a viewing screen. Electromyography can be painful and is less accurate than nerve conduction. Some experts question whether it adds any valuable diagnostic information. They suggest that its use be limited to unusual cases, or when other tests indicate that the condition is aggressive and may increase the risk for rapid, significant injury.
Although electrodiagnostic studies are frequently done to confirm the diagnosis of CTS in patients with classic symptoms, they are also performed on patients with symptoms that do not point to CTS as clearly. Doctors must interpret test results in these patients more carefully.
Portable electrodiagnostic testing
Portable electronic devices are being evaluated for measuring nerve conductivity. They are relatively quick and easy to use on a large scale in an industrial facility. However, these devices have not been not well studied in clinical trials.
Limitations
Electrodiagnostic studies are not well standardized, and certain conditions can skew the results of either test:
- Obesity can slow the speed of electrical conduction.
- Women and the elderly normally have slower conduction times than younger adult men.
A diagnosis of CTS may follow testing the affected hand for numbness, tingling, weakness or pain in specific areas. Muscle and nerve conduction tests may also help affirm or rule out carpal tunnel syndrome.
Treatment
It is critical to begin treating early phases of CTS before the damage progresses. A conservative approach to CTS, which may include corticosteroid injections and splinting, is the first step in treating this disorder. The conservative approach is most successful in patients with mild carpal tunnel syndrome. If the initial treatment doesn't improve symptoms in 2 to 7 weeks, another treatment or surgery should be tried.
Some patients may start with surgery if there is evidence of nerve damage. Studies suggest that surgery is a better option for severe CTS. Surgery improves function and symptoms better than splinting or anti-inflammatory drugs plus hand therapy over the long term. The improvements last for more than 6 months.
Even among patients with mild CTS, there is a high risk of relapse.
Limiting Movement
If possible, the patient should avoid activities at work or home that may aggravate the syndrome. The affected hand and wrist should be rested for 2 to 6 weeks. This allows the swollen, inflamed tissues to shrink and relieves pressure on the median nerve. If the injury is work related, the worker should ask to see if other jobs are available that will not involve the same hand or wrist actions. Few studies have been conducted on ergonomically designed furniture or equipment, or on frequent rest breaks. However, it is reasonable to ask for these if other work is not available.
Conservative Treatment Approach
The following conservative approaches have been shown to provide symptom relief in the short term, although their long-term effectiveness isn't yet known:
- Wrist splints
- Injected or short-term oral corticosteroids
- Ultrasound
Nonsteroidal anti-inflammatory drugs (NSAIDs) may provide short-term relief of symptoms, but have not been found to help the basic problem go away. NSAIDs include common pain relievers such as aspirin and ibuprofen (Advil). Diuretics, magnet therapy, laser acupuncture, vitamin B6, exercise, or chiropractic care also do not help clear up carpal tunnel syndrome. Other approaches being investigated include omega-3 fatty acid supplements.
Underlying Conditions
It is important to treat any underlying medical condition that might be causing carpal tunnel syndrome. For example, reducing inflammation in rheumatoid arthritis or other forms of inflammatory disorders that directly cause CTS is very helpful. Hypothyroidism and diabetes are diseases associated with an increased risk of CTS. The treatments for such diseases may offer some relief for CTS symptoms.
Wrist Splints
Wrist splints can keep the wrist from bending. They are not as beneficial as surgery for patients with moderate-to-severe CTS, but they appear to be helpful in specific patients, such as those with mild-to-moderate nighttime symptoms that have lasted for less than a year.
Typically the splint is worn at night or during sports. The splint is used for several weeks or months, depending on the severity of the problem, and it may be combined with hand and finger exercises. Benefits may last even after the patient stops wearing the splint.
Corticosteroids
Corticosteroid Injections
Corticosteroids (also called steroids) reduce inflammation. If restricting activities and using painkillers are unsuccessful, the doctor may inject a corticosteroid into the carpal tunnel.
In CTS, steroid injections (such as cortisone or prednisolone) shrink the swollen tissues and relieve pressure on the nerve. There is good evidence that they offer short-term symptom relief in a majority of CTS patients. However, in about half of cases, symptoms return within 12 months. Generally a second injection does not provide any added benefit. Another concern with the use of these injections in moderate or severe disease is that nerve damage may occur even while symptoms are improving.
Corticosteroid injections are helpful for pregnant patients, as their symptoms often go away within 6 to 12 months after pregnancy.
Most doctors limit steroid injections to about three per year, because they can cause complications, such as weakened or ruptured tendons, nerve irritation, or more widespread side effects.
Low-Dose Oral Corticosteroids
A short course (1 to 2 weeks) of oral corticosteroid medicines may provide relief for some people, but the relief does not usually last. Long-term use of these medications can cause serious side effects.
Ultrasound
Ultrasound uses high-frequency sound waves directed toward the inflamed area. The sound waves are converted into heat in the deep tissues of the hand, opening the blood vessels and allowing oxygen to be delivered to the injured tissue. Ultrasound is often performed along with nerve and tendon exercises. Ultrasound treatment appears to be effective in the short term, but its long-term benefit remains unknown.
Yoga and Other Exercise Programs
Yoga
Very limited evidence suggests that yoga practice may provide some benefit for patients with carpal tunnel syndrome. Yoga postures are designed to stretch, strengthen, and balance upper body joints.
General Exercise Program
Some experts have reported that people who are physically fit, including athletes, joggers, and swimmers, have a lower risk for cumulative trauma disorders. Although there is no evidence that exercise can directly improve CTS, a regular exercise regimen using a combination of aerobic and resistance training techniques strengthens the muscles in the shoulders, arms, and back; helps reduce weight; and improves overall health and well-being.
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
Nonsteroidal anti-inflammatory drugs (NSAIDs), which include aspirin and ibuprofen (Advil), are the most common pain relievers used for CTS. They block prostaglandins, the substances that dilate blood vessels and cause inflammation and pain. However, there are few well-conducted studies to determine their role in CTS. To date, there is no evidence that they offer any long-term relief, and regular use can have serious side effects. Therefore, NSAIDs are generally not used for the long-term treatment of carpal tunnel symptoms.
Other Conservative Approaches
Ice
Ice may help with acute pain. Some patients have reported that alternating warm and cold soaks is beneficial. (If hot applications relieve pain, most likely the problem is not caused by CTS but by another condition that produces similar symptoms.)
Low-Level Laser Therapy
Some investigators are working with low-level laser therapy (LLLT), which generates extremely pure light in a single wavelength. The procedure is painless. However, 2 trials comparing laser therapy to conservative treatment or a placebo laser treatment found no real benefit from this therapy.
Surgery
Carpal tunnel release surgery is among the most common surgeries performed in the United States. In various trials, 70% to 90% of patients who underwent surgery were free from nighttime pain afterward. Studies have found that surgery provides a greater benefit over the long term compared with splinting or anti-inflammatory drugs plus hand therapy.
Candidates for Surgery
Although evidence strongly suggests that surgery is more effective than conservative approaches (at least in patients with moderate-to-severe CTS), the decision about whether to have surgery to correct CTS, and when to have it, is not always clear. Electrodiagnostic and other tests used to confirm CTS are not always perfect or useful in determining the best candidates for surgery.
As a result, surgery does not cure all patients. A number of experts believe that release surgery is performed too often. Some recommend a full trial of conservative treatment (such as splints, anti-inflammatory agents, and physical therapy) before choosing surgery. Others warn that CTS is often progressive and will worsen over time without surgery, and that surgery is better than splints and conservative measures for pain relief in cases where CTS is likely present.
Factors that may increase the chances of successful surgery
- Having surgery performed within 3 years of being diagnosed with the disorder
- Being in good general health
- Having very slow nerve conduction results, but also having reasonably good muscle strength before surgery
- Having symptoms that are worse at night than during the day
Factors that may reduce the chances for success
Having very severe symptoms before surgery, such as:
- Continual numbness
- Muscle weakness and wasting
- Very poor nerve conduction results
Other symptoms include:
- Symptoms that have been present for more than 10 months.
- Being over 50 years old.
- Performing heavy manual labor, particularly working with vibrating tools. Only slightly more than half of people who use vibrating hand-held tools are symptom-free 3 years after a CTS operation.
- Patients who are on hemodialysis have good initial success, but the condition deteriorates in about half of these patients after around a year and a half.
- Poor mental health or alcohol abuse.
- Patients with diabetes and high blood pressure may be more likely to require a second operation.
- Patients have a work related injury that caused CTS.
Standard Release Surgical Procedures
CTS surgery can be performed through a standard open release, a mini-open technique, or endoscopy. There is no clear evidence to suggest that one surgical technique is much better than another over the long term.
Open Release Surgery
Traditionally, surgery for CTS has involved an open surgical procedure performed in an outpatient facility. In this procedure, the carpal ligament is cut free (released) from the median nerve. This relieves pressure on the median nerve. The surgery is straightforward.
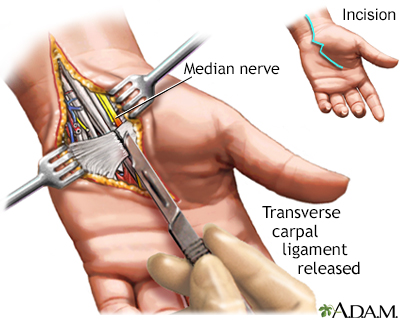
In treating carpal tunnel syndrome, surgery may be required to release the compressed median nerve. The open release procedure involves simply cutting the transverse carpal ligament.
The Mini-Open Approach
In recent years, more surgeons have adopted a "mini" open -- also called short-incision -- procedure. This surgery requires only a 1-inch incision, but it still allows a direct view of the area (unlike endoscopy, which is viewed on a monitor.) The mini-open approach seems to reduce recovery time, pain, and recurrence rate compared to an open approach. However, over the long term there doesn't seem to be any significant difference between the mini-open approach and the standard open release.
Endoscopy
Endoscopy for CTS is a less invasive procedure than standard open release.
- A surgeon makes one or two 1/2-inch incisions in the wrist and palm, and inserts one or two endoscopes (pencil-thin tubes).
- The surgeon then inserts a tiny camera and a knife through the lighted tubes.
- While looking at the underside of the carpal ligament on a screen, the surgeon cuts the ligament to free the compressed median nerve.
Patients who have endoscopic surgery report less pain than those who have the open release procedure, and they return to normal activities in about half the time. Nevertheless, at this time the best evidence available does not show any significant long-term advantages of endoscopy over open release in terms of muscle, grip strength, or dexterity. The endoscopic approach may even carry a slightly higher risk of pain afterward. This may be due to a more limited view of the hand with endoscopy. (In the open release procedure, the surgeon has a full view of the structures in the hand.) Because of this reduced visibility, there are more concerns about irreversible nerve injury with endoscopic carpal tunnel release than with open carpal tunnel release. However, larger studies have shown an extremely low number of complications when the procedure is performed by experienced physicians. The difference in pain is also not that significantly different clinically.
Endoscopic approaches have a faster return to work outcomes when compared with open approaches.
Recovery after Surgery
Timing of Recovery
For some patients, release surgery relieves symptoms of numbness and tingling immediately.
- People who have the operation on both hands will need someone to help them at home for about 2 weeks.
- Returning to strenuous work right after surgery may cause the symptoms to return. Patients who work in strenuous jobs generally stay out of work for at least a month and often much longer, depending upon the type of surgery and the severity of the condition. Recovery time appears to be faster with endoscopy or mini-open release than with open release.
- People who perform light office work will return to work much sooner, although possibly with some limitations.
- Immediately after surgery, patients usually experience a decline in grip strength and dexterity. Studies have reported a wide range of recovery in this area. The scar may remain tender for up to a year.
- Peak improvement (the best level of improvement a patient can reach) may take a long time (up to 10 months).
Physical Therapy
Physical therapy following surgery has not been shown to speed up recovery or affect the final outcome of CTS surgery.
Complications and Long-Term Outcome
Treatment failure and complication rates of CTS surgery vary.
Complications after surgery may include the following:
- Nerve damage with tingling and numbness (usually temporary).
- Infection.
- Scarring.
- Pain.
- Stiffness.
- Complex regional pain syndrome - increased pain sensitivity.
- Loss of some wrist strength is a complication that affects some patients. Some patients who have jobs requiring significant hand and wrist strength may not be able to perform them after surgery. These workers may also have problems in other parts of the upper body, including the elbows and shoulders. These problems do not go away with surgery and can persist.
If pain and symptoms return, the release procedure may be repeated.
Reasons for procedure failure include:
- Incomplete release of the ligament
- Extensive scarring
- Recurrence of the disorder due to underlying medical conditions
Resources
- American Association of Neuromuscular and Electrodiagnostic Medicine -- www.aanem.org/Home
- American Physical Therapy Association -- www.apta.org
- Association of Occupational and Environmental Clinics -- www.aoec.org
- American Academy of Orthopaedic Surgeons -- www.aaos.org
- American Society for Surgery of the Hand -- www.assh.org/s
- International Association for the Study of Pain -- www.iasp-pain.org
- American Academy of Neurology -- www.aan.com
- National Institute of Arthritis and Musculoskeletal and Skin Diseases -- www.niams.nih.gov
- National Institute of Neurological Disorders and Stroke -- www.ninds.nih.gov
- Information on CTS -- medlineplus.gov/carpaltunnelsyndrome.html
- National Institute for Occupational Safety and Health -- www.cdc.gov/niosh
References
Calandruccio JH. Carpal tunnel syndrome, ulnar tunnel syndrome, and stenosing tenosynovitis. In Azar FM, Beaty JH, Canale ST, eds. Campbell's Operative Orthopaedics. 13th ed. Philadelphia, PA: Elsevier; 2017:chap 76.
Dyer GSM, Simmons BP. The wrist and hand. In: Hochberg MC, Gravallese EM, Silman AJ, Smolen JS, Weinblatt ME, Weisman MH, eds. Rheumatology. 7th ed. Philadelphia, PA: Elsevier; 2019:chap 84.
Erickson M, Lawrence M, Jansen CWS, Coker D, Amadio P, Cleary C. Hand pain and sensory deficits: carpal tunnel syndrome. J Orthop Sports Phys Ther. 2019;49(5):CPG1-CPG85. PMID: 31039690 www.ncbi.nlm.nih.gov/pubmed/31039690.
Graham B, Peljovich AE, Afra R, et al. The American Academy of Orthopaedic Surgeons evidence-based clinical practice guideline on: management of carpal tunnel syndrome. J Bone Joint Surg Am. 2016;98(20):1750-1754. PMID: 27869627 www.ncbi.nlm.nih.gov/pubmed/27869627.
Huisstede BM, van den Brink J, Randsdorp MS, Geelen SJ, Koes BW. Effectiveness of surgical and postsurgical interventions for carpal tunnel syndrome-a systematic review. Arch Phys Med Rehabil. 2017. PMID: 28577858 www.ncbi.nlm.nih.gov/pubmed/28577858.
Kleopa KA. In the clinic. Carpal tunnel syndrome. Ann Intern Med. 2015;163(5):ITC1. PMID: 26322711 www.ncbi.nlm.nih.gov/pubmed/26322711.
Mooar PA, Doherty WJ, Murray JN, Pezold R, Sevarino KS. Management of carpal tunnel syndrome. J Am Acad Orthop Surg. 2018;26(6):e128-e130. PMID: 29420323 www.ncbi.nlm.nih.gov/pubmed/29420323.
Padua L, Coraci D, Erra C, et al. Carpal tunnel syndrome: clinical features, diagnosis, and management. Lancet Neurol. 2016;15(12):1273-1284. PMID: 27751557 www.ncbi.nlm.nih.gov/pubmed/27751557.
Page MJ, O'Connor D, Pitt V, Massy-Westropp N. Therapeutic ultrasound for carpal tunnel syndrome. Cochrane Database Syst Rev. 2013;(3):CD009601. PMID: 23543580 www.ncbi.nlm.nih.gov/pubmed/23543580.
Ronthal M. Arm and neck pain. In: Daroff RB, Jankovic J, Mazziotta JC, Pomeroy SL. Bradley's Neurology in Clinical Practice. 7th ed. Philadelphia, PA: Elsevier; 2016:chap 31.
Vasiliadis HS, Georgoulas P, Shrier I, Salanti G, Scholten RJ. Endoscopic release for carpal tunnel syndrome. Cochrane Database Syst Rev. 2014;(1):CD008265. PMID: 24482073 www.ncbi.nlm.nih.gov/pubmed/24482073.
Wipperman J, Goerl K. Carpal tunnel syndrome: diagnosis and management. Am Fam Physician. 2016;94(12):993-999. PMID: 28075090 www.ncbi.nlm.nih.gov/pubmed/28075090.
|
Review Date:
12/2/2019 Reviewed By: C. Benjamin Ma, MD, Professor, Chief, Sports Medicine and Shoulder Service, UCSF Department of Orthopaedic Surgery, San Francisco, CA. Also reviewed by David Zieve, MD, MHA, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. |
 All rights reserved.
All rights reserved.