

Periodontal Disease - InDepth
Highlights
Symptoms of Periodontal Disease
Symptoms of periodontal disease include red and swollen gums, gums that bleed while brushing, persistent bad breath, receding gums, and loose teeth. Smoking, certain illnesses (such as diabetes), older age, stress, and other factors increase the risk for periodontal disease.
If you have periodontal disease, your dentist may refer you to a periodontist, a dentist who specializes in treating this condition. Without proper treatment, periodontal disease can lead to tooth loss.
Prevent Periodontal Disease: Practice Good Dental Hygiene
Consistent good dental hygiene can help prevent gingivitis and periodontitis. If you smoke, you should quit. Smoking is a major risk factor for gum disease. The American Dental Association recommends that everyone:
- Brush twice daily with a fluoride toothpaste (be sure to replace toothbrushes every 1 to 3 months).
- Clean between the teeth with floss or an interdental cleaner.
- Eat a well-balanced diet and limit snacking between meals.
- Have regular visits with a dentist for teeth cleaning and oral examinations.
Treatment
Scaling and root planing is the first approach for treating periodontal disease. This procedure is a deep cleaning to remove bacterial plaque and calculus (tartar). Scaling involves scraping tartar from above and below the gum line. Root planing will smooth the root surfaces of the teeth. Your dentist will reevaluate the success of this treatment in follow-up visits. If deep periodontal pockets and infection remain, periodontal surgery may be recommended.
Periodontal Disease and Heart Disease
Periodontal disease and heart disease share certain common risk factors, such as smoking and diabetes. Untreated or inadequately controlled moderate-to-severe periodontal disease may increase the risk for heart disease. However, according to the American Heart Association:
- There is no definitive proof that gum disease causes heart disease and stroke.
- There is no definitive proof that treating gum disease can help prevent heart disease and stroke.
- More evidence is needed to establish a cause-and-effect relationship between these conditions.
In general, periodontists and cardiologists recommend that:
- People who have periodontal disease and at least one risk factor for heart disease should have a medical evaluation for heart problems.
- People who have heart disease should have regular exams to check for signs of periodontal disease.
Introduction
Periodontal disease is disease of both gums and bone. The word "periodontal" means "around the tooth." Periodontal disease is an inflammatory disease of the tissues that surround and support the teeth. These include the gingiva (or gums), bone, and supporting ligaments that connect from the bone to the teeth (PDL). If left untreated, periodontal disease will lead to bone loss, which can lead to tooth loss.
The Periodontium
The periodontium is the part of the mouth that consists of the gum and supporting structures. It is made up of the following parts:
Gingiva (gum).
When healthy, the gingiva is pale pink, firm, and does not move. It has a smooth or speckled texture (called stippling). The gingival tissue between teeth is shaped like a wedge.Sulcus (pocket).
The sulcus is the space between the gum and tooth. In health it measures from 1mm to 3 mm in depth and bathes the tooth in special fluids called crevicular fluids. It is also the main place where periodontal problems begin.Cementum.
This is the name given to the surface of the roots of the teeth.Periodontal ligament.
This thin ligament is a specialized connective tissue that connects the cementum and the alveolar bone.Alveolar bone.
The alveolar bone contains the teeth sockets and supports the teeth.
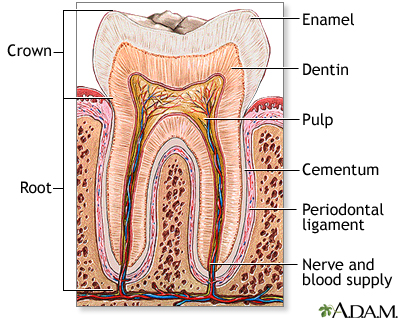
The structure of the tooth includes outer layers made of enamel and cementum. The inner layers include dentin, pulp and other tissues, blood vessels, and nerves. The cementum covers the root and is embedded in the bony jaw. Above the gum line, the tooth is protected by the hard enamel shell.
Periodontal Disease
Periodontal diseases are generally divided into two groups:
Gingivitis.
Caused by inflammatory lesions that affect the gums, is a milder form of gum disease.Periodontitis.
Which involves damage to the bone and connective tissue that support the teeth, is a more serious form of gum disease.

Click the icon to see an image of gingivitis.
Gingivitis
Gingivitis is an inflammation of the gingiva, or gums. It is characterized by tender, red, swollen gums that bleed easily and may cause bad breath (halitosis). Gingivitis can be treated by good dental hygiene, proper diet, and stopping smoking. Untreated gingivitis can lead to periodontitis.
The Periodontitis
Periodontitis is an inflammation of the supporting tissues of teeth that occurs when the gum tissues separate from the tooth and sulcus, forming periodontal pockets. Periodontitis is characterized by:
- Gum inflammation, with redness, puffiness, and bleeding
- Deep pockets (normal depth is between 1 and 3 millimeter) that form between the gum and the tooth
- Loose teeth
- Bad breath (halitosis)
There are different forms of periodontal disease. In 2017, the American Academy of Periodontology has adopted a new classification scheme for periodontal disease. The new classification has eliminated the distinction previously made between chronic periodontitis and aggressive periodontitis. Current periodontitis forms include:
Periodontitis
Periodontitis is defined based on its severity and complexity. As the disease progresses, the periodontal support around teeth is gradually lost. This tissue loss is measured and used to assess the stage of periodontitis.
Disease-Related Periodontitis (Periodontitis as a Manifestation of Systemic Disease)
Periodontitis can also be associated with a number of systemic diseases, including type 1 and type 2 diabetes, Down syndrome, AIDS, rheumatoid arthritis, and several rare disorders of white blood cells.
Necrotizing Periodontal Disease
Acute necrotizing ulcerative gingivitis (ANUG) is an uncommon acute infection of the gum tissue. It is characterized by painful and bleeding gums, bad breath, and rapid onset of pain. If left untreated, necrotizing periodontal disease can spread throughout the facial areas (cheeks, jaw) and cause extensive damage. Necrotizing periodontal disease is usually associated with stress or systemic health conditions such as AIDS and malnutrition.
Causes
Periodontal disease is caused by dental
plaque
, which contains harmful bacteria. The mouth is full of bacteria but they tend to be harmless varieties. Periodontal disease usually develops because of an increase in bacteria quantity in the oral cavity and a change in balance from harmless to disease-causing bacteria. These harmful bacteria increase in mass and thickness until they form a sticky residue called plaque.Plaque begins to form within a minute after you finished brushing your teeth. Plaque is a type of
biofilm
, composed of bacteria encased in a sticky extracellular matrix. When plaque growth accumulates to excessive levels, it will cause inflammation and infection of periodontal structures.When plaque is allowed to remain in the periodontal area, it becomes mineralized and transforms into
calculus
(commonly known astartar
). This material has a rock-like consistency and grabs onto the tooth surface. Tartar is much more difficult to remove than plaque, which is a soft mass. Once tartar has formed, it must be professionally removed by a dental practitioner.Risk Factors
Most adults have some form of gum disease but are unaware of it. The main risk factors for periodontal disease include:
- Smoking or tobacco use
- Age
- Female hormonal changes
- Stress
- Medications
- Chronic health conditions
- Genetic factors
Age
Periodontitis typically occurs as people get older and is most common after age 35.
Lifestyle Factors
Smoking
Smoking is the major preventable risk factor for periodontal disease. Smoking can cause bone loss and gum recession even in the absence of periodontal disease. The risk for periodontal disease increases with the number of cigarettes smoked per day. Smoking cigars and pipes carries the same risks as smoking cigarettes.
Smokeless tobacco
Smokeless tobacco will cause localized damage to gums in the area where the tobacco is held in the mouth. It will also change the soft tissue cells to become pre-cancerous. Smokeless tobacco may cause oral cancer.
Substance abuse
Long-term abuse of alcohol and certain types of illegal drugs (amphetamines) can damage gums and teeth.
Diet
Malnutrition is a risk factor for periodontal disease. A healthy diet, including eating fruits and vegetables rich in vitamin C, is important for good oral health.
Stress
Psychological stress can cause the body to release inflammatory hormones that may trigger or worsen periodontal disease. In addition, when people are feeling stressed out they tend to take poorer care of their health, including regular brushing and flossing.
Female Hormones
Female hormones affect the gums, and women in particular are susceptible to periodontal problems.
Menstruation
Gingivitis may flare up in some women a few days before they menstruate, when progesterone levels are high. Gum inflammation may also occur during ovulation. The female hormone progesterone dilates blood vessels, which causes inflammation and blocks the repair of collagen, the structural protein that supports the gums.
Pregnancy
Hormonal changes during pregnancy can cause gingivitis or aggravate existing gingivitis. Gingivitis typically worsens around the second month of pregnancy and reaches a peak in the eighth month. Pregnancy-related gingivitis usually resolves within a few months of delivery. Because periodontal disease may increase the risk for low-weight infants and cause other complications, it is important for pregnant women to see a dentist.
Menopause
Estrogen deficiency after menopause reduces bone mineral density, which can lead to bone loss. Bone loss is associated with both periodontal disease and osteoporosis (loss of bone density). The hormonal changes associated with menopause can cause dry mouth (xerostomia), which can lead to tooth and gum problems.
Genetic Factors
Periodontal disease often occurs in members of the same family. Genetic factors play a role in making some people more susceptible to periodontal disease. This is most true with aggressive periodontitis. If one child is found to have periodontal disease, all siblings should be checked for the disease.
Medical Conditions Associated with Periodontal Disease
Diabetes
There is a strong two-way association between diabetes (both type 1 and 2) and periodontal disease. People with diabetes who have poorly controlled blood sugar (glucose) levels are at high risk of developing many kinds of infections, including periodontal disease. There is also evidence that periodontal disease may adversely affect blood sugar (glycemic) control, which can increase the risk for other health complications.
Heart Disease
Periodontal disease and heart disease share common risk factors (smoking, older age, diabetes) but it is not yet clear if having one condition increases the risk of developing the other (see Complications section of this report).
Other Medical Conditions
A number of medical conditions can increase the risk of developing gingivitis and periodontal disease. They include conditions that affect the immune system such as HIV/AIDS, leukemia, Down syndrome, and autoimmune disorders (Crohn disease, multiple sclerosis, systemic lupus erythematosus). There is also evidence that severe periodontal disease may increase the risk of developing certain autoimmune disorders, such as rheumatoid arthritis.
Prescription Medications
Gingival overgrowth can be a side effect of many drugs including certain types of oral contraceptives, antidepressants, and heart medications. Any drug that has a side effect of dry mouth can increase the risk for gum disease.
If you take a bisphosphonate drug such as alendronate (Fosamax) discuss with your dentist any potential risks from dental procedures (such as extractions and implants) that involve the jawbone.
Oral bisphosphonates, which are used to treat osteoporosis, have in rare cases caused osteonecrosis (bone destruction) of the jaw. (Intravenous bisphosphonates, which are used in cancer treatment, are more likely to cause osteonecrosis.) Your dentist or oral surgeon may need to take special precautions when performing dental surgery. In any case, be sure to inform your dentist of all medications you take.
Oral Health Risk Factors
Oral Hygiene
Lack of oral hygiene, such as not brushing or flossing regularly, encourages bacterial buildup and plaque formation.
Poorly Contoured Restorations
Poorly contoured restorations (fillings or crowns) that provide traps for debris and plaque can also contribute to periodontitis.
Tooth Structure
Abnormal tooth structure can increase the risk for periodontal disease.
Wisdom Teeth
Wisdom teeth, also called third molars, can be a major breeding ground for the bacteria that cause periodontal disease. Periodontitis can occur in wisdom teeth that have broken through the gum as well as teeth that are impacted (buried). Adolescents and young adults with wisdom teeth should have a dentist check for signs of periodontal disease.
Complications
Effect on Heart Disease
Researchers are studying the association between periodontal disease and heart disease. These two conditions share common risk factors (such as smoking and diabetes). However, some studies suggest that the link between periodontal disease and heart disease involves more than shared risk factors. An inflammatory response, which occurs in both periodontal disease and heart disease, may be the common element.
According to the American Heart Association, there is currently not enough evidence to prove that periodontal disease increases the risk for heart disease or stroke, or that treating gum disease can help prevent these cardiac conditions. The U.S. Preventive Services Task Force does not recommend including periodontal disease among the factors used for estimating a healthy person's risk of developing heart disease.
Cardiologists and periodontists currently encourage each other to monitor both conditions in their patients. Periodontists recommend that people who have periodontal disease and at least one risk factor for heart disease have an annual medical exam to check their heart health. Cardiologists suggest that people with atherosclerosis and heart disease have regular periodontal exams.
Effect on Diabetes
Diabetes is not only a risk factor for periodontal disease. Periodontal disease itself can worsen diabetes, both type 1 and type 2, and make it more difficult to control blood sugar.
Effect on Respiratory Disease
Bacteria that reproduce in the mouth can also be carried into the airways in the throat and lungs, increasing the risks for respiratory diseases such as pneumonia. These bacteria can also worsen chronic lung conditions such as emphysema.

Click the icon to see an image of emphysema.
Effect on Pregnancy
Bacterial infections that cause moderate-to-severe periodontal disease in pregnant women may increase the risk for premature delivery and low birth weight infants. The bacteria from gum disease and tooth decay may trigger the same factors in the immune system that cause premature dilation and contractions.
Women should have a periodontal examination before becoming pregnant or as soon as possible thereafter. Because women with diabetes are at higher risk for periodontal disease, it is especially important that they see a dentist early in pregnancy. Doctors are still not sure if treating periodontal disease can improve birth outcomes. In any case, periodontal treatment is safe for pregnant women.
Symptoms
Symptoms or periodontal disease typically progress over time and include:
Red and Swollen Gums.
These are one of the first signs of periodontal disease.Gum Bleeding.
Bleeding of the gums, even during brushing, is a sign of inflammation and the major marker of periodontal disease.Bad Breath.
Debris and bacteria can cause a bad taste in the mouth and persistent bad breath.Gum Recession and Loose Teeth.
As the disease advances, the gums recede, and the supporting structure of bone is lost. Teeth loosen, sometimes causing a change in the way the upper and lower teeth fit together when biting down or how partial dentures fit.Abscesses.
Deepening periodontal pockets between the gums and bone can become blocked by tartar or food particles. Infection-fighting white blood cells become trapped and die; pus forms, and an abscess develops. Abscesses can destroy both gum and tooth tissue, cause nearby teeth to become loose and painful, and may cause fever and swollen lymph nodes.

Abnormally bulging, protruding, or swollen gums are a possible sign of disease.

Click the icon to see an image of recessed gums.

Click the icon to see an image of a tooth abscess.
Pain is usually not a symptom, which partly explains why the disease may become advanced before treatment is sought and why some people avoid treatment even after periodontitis is diagnosed.
Diagnosis
The dental practitioner typically performs a number of procedures during a routine dental exam to check for periodontal disease. If periodontal disease is suspected, your dentist may refer you to see a periodontist. A periodontist is a dentist who specializes in the diagnosis and treatment of periodontal disease.
Medical History
The dentist will first take a medical history to reveal any past or present periodontal problems, and any medications or underlying diseases that might be contributing to the problem. The dentist will also ask questions about your daily oral hygiene regimen (brushing, flossing).
Oral Examination
Inspection of the Gum Area
The dentist inspects the color and shape of gingival tissue on the cheek (buccal) side and the tongue (lingual) side of every tooth. Redness, puffiness, and bleeding upon probing indicate inflammation and possible periodontal disease.
Periodontal Screening and Recording (PSR)
PSR is a procedure used to measure and determine the severity of periodontal disease:
- The dentist uses a mirror and a periodontal probe, a thin instrument calibrated in millimeters (mm), which is used to measure pocket depth.
- The probe is held along the length of the tooth with the tip placed into the pocket. The tip of the probe will then touch the bottom of the pocket.
- The dentist will "walk" the probe to 6 specified points on each tooth, 3 on the buccal (cheek), and 3 on the lingual (tongue) sides. The dentist measures the depth of the probe at each point.
- Pocket depths greater than 4 mm indicate disease.
These measurements help determine the condition of the connective tissue and amount of gingival overgrowth or recession.
Testing Tooth Movement
Tooth mobility is determined by pushing each tooth between two instrument handles and observing any movement. Mobility is a strong indicator of bone support loss.
X-rays
X-rays are taken to show any loss of bone structure supporting the teeth.
Treatment
According to the American Academy of Periodontology, treatment for periodontal disease should focus on achieving oral health in the least invasive and most cost-effective manner. Your dentist or periodontist will usually begin with a non-surgical approach (scaling and root planing), then reevaluate your condition in follow-up visits. If infection or deep periodontal pockets remain, surgical treatment may be recommended.
Periodontal treatment approaches can basically be categorized as:
Nonsurgical Approaches.
Scaling and root planing (deep cleaning of tartar and bacteria from gum line and tooth root surfaces), which may include the use of topical or systemic antibiotics.Surgical Approaches.
Periodontal surgical techniques include flap surgery (periodontal pocket reduction with or without the use of a laser -- LANAP), gum grafts, bone grafts, and guided tissue regeneration.Restorative Procedures.
Crown lengthening is an example of a restorative procedure that may be performed for cosmetic reasons or to improve function. For people who have already lost teeth to advanced periodontitis, dental implants are another option.
In addition to treatment in a dentist office, regular dental visits and cleanings (usually every 3 months for the first year and every 4 to 6 months thereafter, if the disease is eradicated) are important for maintenance as is practicing good oral hygiene at home.
Non-Surgical Treatment
Scaling and Root Planing
Scaling and root planing is a deep cleaning to remove bacterial plaque and calculus (tartar). It is the cornerstone of periodontal disease treatment and the first procedure a dentist will use. Scaling involves scraping tartar from above and below the gum line. Root planing will smooth the root surfaces of the teeth.
The dentist may apply a topical anesthetic or inject a local anesthetic to numb the area before beginning the procedure. Both ultrasonic and manual instruments are used to remove calculus. The ultrasonic device vibrates at a high frequency and helps loosen and remove calculus. A high-pressure water spray is then used to flush out the debris.
The dentist will use manual instruments called scrapers and curettes to scrape away any remaining plaque or calculus and smooth and clean the tooth crown and root surfaces. Finally, the dentist will polish the tooth using abrasive paste that also has fluoride applied to a spinning instrument with a rubber cap. Polishing produces a smooth surface, making it temporarily harder for plaque to adhere.
Antibiotics
At the time of scaling and root planing, your dentist may recommend the use of antibiotic medications.
Antibiotics for periodontal disease come in various forms. They may be taken as a prescription mouthwash rinse or placed topically directly into the pockets being treated as dissolving gels, threads, or microchips into the periodontal pockets. In some cases, the dentist may prescribe a short course of systemic antibiotics with low-dose tetracycline, doxycycline, or amoxicillin with metronidazole.
Surgical Treatment
Flap Surgery (Periodontal Pocket Reduction)
Surgery allows access for deep cleaning of the root surface, removal of diseased tissue, and repositioning and shaping of the bones, gum, and tissues supporting the teeth. The basic procedure is known as flap surgery. It is performed under local anesthesia and involves:
- The periodontist makes an incision and folds back the gum surface away from the tooth and surrounding bone.
- The diseased root surfaces are cleaned and curetted (scraped) to remove deposits.
- Gum tissue is sewn back into a position to minimize pocket depth.
- The periodontist may also contour the remaining bone or attempt to regenerate lost bone and gingival attachment through bone grafts or guided tissue regeneration.
For several days following surgery, you should rinse your mouth with warm salt water to help reduce swelling. Post-surgical discomfort is usually treated with over-the-counter medications such as ibuprofen or the application of ice packs.
Gum Graft
In cases of excessive gingival recession, the periodontist may perform a gum (gingival) graft to cover the area of exposed root. There are various ways to perform the tissue graft:
Free gingival graft.
Removes a thin layer of tissue from the palate of the mouth and sutures onto the exposed root surface. However, many people find the healing of the donor site on the roof of the mouth to be more painful than the actual surgical procedure.Subepithelial connective tissue graft.
Removes tissue from inside the palate (as opposed to the outside, as with the free gingival graft). Recovery is less painful with this method.Acellular allograft dermal matrix.
Uses specially processed tissue derived from donated cadavers. No tissue is taken from the patient.
A synthetic graft has also been developed, however, various studies have shown that bone additives and growth factors give better results than synthetic grafts.
Bone Graft
In some cases of severe bone loss, the surgeon may attempt to encourage regrowth and restoration of bone tissue that has been lost through the disease process. This involves bone grafting:
- The surgeon places bone graft material into the defective area.
- The material may come from the patient (autogenous), from a cadaver (allograft), or from an animal such as a cow (xenograft). An autogenous graft is considered the best approach.
- The gum is then sewn back into place.
- During the next 6 to 9 months, the bone regrows in the jaw area helping to reattach the teeth to the jaw.
Guided tissue regeneration is a more advanced technique that may be used along with bone grafting:
- A specialized piece of fabric called a barrier membrane is placed between the gum and the existing bone defect.
- The gum is then sewn over the fabric. The fabric prevents the gum tissue from growing down into the bone defect and allows the bone and the attachment to the root to regenerate.
Restorative and Cosmetic Treatments
Crown lengthening
A surgical procedure performed to expose more of the tooth. It involves readjusting the gum and bone levels by removing small sections of bone and resewing the gums into a new position to allow more tooth exposure.
Dental implants
An option for people who have lost teeth to periodontal disease. Dental implants are an artificial type of tooth root used for permanent prosthetic teeth. Implants are screws placed into the jawbone. Prosthetic teeth are attached to the implants.
Prevention
In addition to regular visits to a dentist, the best prevention for periodontal disease takes place at home. Healthy habits and good oral hygiene, including daily brushing and flossing, are critical in preventing gum disease and maintaining good oral health after periodontal treatment.
Tooth Brushing
Correct tooth brushing is the first defense against periodontal disease. Here are some tips for brushing correctly:
- Use a soft-bristled brush that fits the size and shape of your mouth.
- Place the brush where the gum meets the tooth, with bristles resting along each tooth at a 45-degree angle.
- Move the brush back and forth gently. Use short vertical or circular strokes. Do not brush horizontally along the tooth.
- Begin by brushing the outer tooth surfaces, followed by the inner tooth surfaces, and then the chewing surfaces of the teeth.
- Brush your tongue to help remove additional bacteria.
- Flossing should finish the process. A mouthwash may also be used.
If brushing after each meal is not possible, rinsing the mouth with water after eating can help reduce bacteria.
Toothbrushes
A vast assortment of brushes of varying sizes and shapes are available, and each manufacturer makes its claim for the benefits of a particular brush. Look for the American Dental Association (ADA) seal on both electric and regular brushes.
Electric toothbrushes, particularly those with a stationary grip and revolving tufts of bristles, can be helpful, especially for people with physical disabilities. However, in general, studies have reported no major differences between electric and manual toothbrushes in their ability to remove plaque. If a regular toothbrush works, it isn't absolutely necessary to buy an electric one.
The major benefit of electric toothbrushes is that you do not have to be a good brusher to remove the plaque. The other benefit is that most electric brushes have a built-in timer, which identifies when the recommended time to brush your teeth (2 minutes) is up. Most people who brush manually do not brush their teeth long enough.
The most important factor in buying any toothbrush, whether electric or manual, is to choose one with a soft head. Soft bristles get into crevices easier, do not irritate the gums and are gentler on the enamel, thereby reducing the risk of exposing the inner layer of dentin or the roots of the teeth below the gum line compared to hard brushes.
Be sure to rinse your toothbrush with water after each use. Toothbrushes should be replaced every 1 to 3 months. Worn bristles are less effective at removing plaque, and old toothbrushes may become breeding grounds for bacteria. To prevent the spread of infection, never share toothbrushes.
Flossing
The use of dental floss, either waxed or unwaxed, is critical in cleaning between the teeth where the toothbrush bristles cannot reach. You can floss before or after brushing; what is important is to floss daily. To floss correctly:
- Break off about 18 inches of floss and wind most of it around the middle finger of one hand and the rest around the other middle finger.
- Hold the floss between the thumbs and forefingers and gently guide and rub it back and forth between the teeth.
- When it reaches the gum line, the floss should be curved around each tooth and slid gently up and down against the tooth.
If you have trouble flossing, some devices may help:
- A floss threader may be helpful for people who have bridgework. Made of plastic, it looks like a needle with a huge eye, or loop. A piece of floss is threaded into the loop, which can then be inserted between the bridge and the gum. The floss that is carried through with it can then be used to clean underneath the false tooth or teeth and along the sides of the abutting teeth.
- An interdental cleaner (Proxabrush) is a tiny narrow brush that can be worked in between the natural teeth or around an attached false tooth.
- Special toothpicks such as Stim-U-Dents may be used for wide spaces between teeth but should never replace flossing. Standard toothpicks should never be used for regular hygiene.
- An electric waterpik delivers a steady jet of water and can help remove plaque build-up between teeth.
Toothpastes and Mouthwashes
Toothpaste
Toothpastes are a combination of abrasives, binders, colors, detergents, flavors, fluoride, humectants, preservatives, and artificial sweeteners. Avoid highly abrasive toothpastes, especially if your gums have receded. The objective of a good toothpaste is to reduce the development of plaque and eliminate periodontitis-causing bacteria.
Ingredients contained in toothpastes may include:
Fluoride.
Most commercial toothpastes contain fluoride, which both strengthens tooth enamel against decay and enhances remineralization of the enamel. Fluoride also inhibits acid-loving bacteria, especially after eating, when the mouth is more acidic. This antibacterial activity may help control plaque.Triclosan.
Triclosan is an anti-bacterial substance that may help reduce mild gingivitis.Metal salts.
Metal salts, such as stannous and zinc, serve as anti-bacterial substances in toothpastes. Stannous fluoride gel toothpastes do not reduce plaque, even though they have some effect against the bacteria that cause it, but slightly reduce gingivitis.Peroxide and baking soda.
Toothpastes with these ingredients claim to have a whitening action, but while they may help remove stains there is little evidence they whiten the actual color of the teeth. In addition, these substances do not appear to offer much protection against gum disease.Antibacterial sugar substitutes
(xylitol), anddetergents
(delmopinol).
Mouthwash
Antimicrobial mouthwashes help prevent and reduce plaque and gingivitis. Fluoride mouthwashes help provide additional protection against tooth decay:
- Antimicrobial mouthwashes, such as Listerine, reduce plaque and gingivitis. Chlorhexidine (Peridex or PerioGard) is an antimicrobial mouthwash available only by prescription to specifically target gingivitis-causing bacteria. It is often prescribed before or following periodontal surgery. Chlorhexidine can temporarily stain teeth. It is typically recommended to rinse for a full 30 seconds to achieve a clinical benefit with these antimicrobial rinses.
- Fluoride mouthwashes (Act) are helpful in preventing cavities.
- Breath-freshening mouthwashes containing cetylpyridinium chloride (Scope, Cepacol, generics) have limited effects on plaque.
- Mouthwashes that contain alcohol (such as certain Listerine products) are dangerous for children under age 12 years. Fluoride mouthwashes should not be used by children younger than age 6 years.
Lifestyle Changes
Eat Healthy
A well-balanced and nutritious diet is important for good oral health. Limit sugary foods and between-meal snacks. Be sure to brush and floss after every meal. It is also important to drink lots of water to help increase saliva and flush away plaque.
Quit Smoking
Smoking, and any kind of tobacco use, is a main risk factor for periodontal disease. For smokers, quitting is one of the most important steps toward regaining periodontal health.
Relieve Stress
Try to incorporate relaxation technique or other stress management strategies into your life. Emotional and psychological stress play a role in periodontal disease.
Resources
- National Institute of Dental and Craniofacial Research -- www.nidcr.nih.gov
- American Academy of Periodontology -- www.perio.org
- American Dental Association -- www.ada.org/en
- American Association of Oral and Maxillofacial Surgeons -- www.aaoms.org
References
Aarabi G, Eberhard J, Reissmann DR, Heydecke G, Seedorf U. Interaction between periodontal disease and atherosclerotic vascular disease--fact or fiction? Atherosclerosis. 2015;241(2):555-560. PMID: 26100678 www.ncbi.nlm.nih.gov/pubmed/26100678.
Camargo PM, Takei HH, Carranza FA. Bone loss and patterns of bone destruction. In: Newman MG, Takei HH, Klokkevold PR, Carranza FA, eds. Newman and Carranza's Clinical Periodontology. 13th ed. Philadelphia, PA: Elsevier; 2019:chap 24.
Caton JG, Armitage G, Berglundh T, et al. A new classification scheme for periodontal and peri-implant diseases and conditions - Introduction and key changes from the 1999 classification. J Periodontol. 2018;89 Suppl 1:S1-S8. PMID: 29926946 www.ncbi.nlm.nih.gov/pubmed/29926946.
Chapple IL, Genco R; Working group 2 of the joint EFP/AAP workshop. Diabetes and periodontal diseases: consensus report of the joint EFP/AAP workshop on periodontitis and systemic diseases. J Clin Periodontol. 2013;84(4 Suppl):S106-S112. PMID: 23631572 www.ncbi.nlm.nih.gov/pubmed/23631572.
Dhar V. Periodontal diseases. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 339.
Dommisch H, Kebschull M. Chronic periodontitis. In: Newman MG, Takei HH, Klokkevold PR, Carranza FA, eds. Newman and Carranza's Clinical Periodontology. 13th ed. Philadelphia, PA: Elsevier; 2019:chap 27.
Herrera D, Retamal-Valdes B, Alonso B, Feres M. Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endo-periodontal lesions. J Periodontol. 2018;89 Suppl 1:S85-S102. PMID: 29926942 www.ncbi.nlm.nih.gov/pubmed/29926942.
Javed F, Warnakulasuriya S. Is there a relationship between periodontal disease and oral cancer? A systematic review of currently available evidence. Crit Rev Oncol Hematol. 2016;97:197-205. PMID: 26343577 www.ncbi.nlm.nih.gov/pubmed/26343577.
Klokkevold PR, Carranza FA. Necrotizing ulcerative periodontitis. In: Newman MG, Takei HH, Klokkevold PR, Carranza FA, eds. Newman and Carranza's Clinical Periodontology. 13th ed. Philadelphia, PA: Elsevier; 2019:chap 29.
Mark AM. Diabetes and oral health. J Am Dent Assoc. 2016;147(10):852. PMID: 27528509 www.ncbi.nlm.nih.gov/pubmed/27528509.
National Institute of Dental and Cranofacial Research website. Periodontal (gum) disease: causes, symptoms, and treatments. www.nidcr.nih.gov/health-info/gum-disease/more-info. Updated July 2018. Accessed August 12, 2019.
Perry DA. Epidemiology of periodontal diseases. In: Perry DA, Beemsterboer PL, Essex G, eds. Periodontology for the Dental Hygienist. 4th ed. St Louis, MO: Elsevier Saunders; 2014:chap 3.
Perry DA, Takei HH, Do JH. Plaque biofilm control for the periodontal patient. In: Newman MG, Takei HH, Klokkevold PR, Carranza FA, eds. Newman and Carranza's Clinical Periodontology. 13th ed. Philadelphia, PA: Elsevier; 2019:chap 48.
Preshaw PM, Chambrone L, Holliday R. Smoking and periodontal disease. In: Newman MG, Takei HH, Klokkevold PR, Carranza FA, eds. Newman and Carranza's Clinical Periodontology. 13th ed. Philadelphia, PA: Elsevier; 2019:chap 12.
Rosenberg ES, Torosian J. Esthetics and periodontics. In: Aschheim KW, ed. Esthetic Dentistry: A Clinical Approach to Techniques and Materials. 3rd ed. St Louis, MO: Elsevier Mosby; 2015:chap 14.
Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J Periodontol. 2018;89 Suppl 1:S159-S172. PMID: 29926952 www.ncbi.nlm.nih.gov/pubmed/29926952.
Tonetti MS, Van Dyke TE; Working group 1 of the joint EFP/AAP workshop. Periodontitis and atherosclerotic cardiovascular disease: consensus report of the Joint EFP/AAP workshop on periodontitis and systemic diseases. J Clin Periodontol. 2013;40 Suppl 14:S24-S29. PMID: 23627332 www.ncbi.nlm.nih.gov/pubmed/23627332.
Touger-Decker R, Mobley C; Academy of Nutrition and Dietetics. Position of the Academy of Nutrition and Dietetics: oral health and nutrition. J Acad Nutr Diet. 2013;113(5):693-701. PMID: 23601893 www.ncbi.nlm.nih.gov/pubmed/23601893.
U.S. Department of Health and Human Services Federal Panel on Community Water Fluoridation. U.S. Public Health Service Recommendation for fluoride concentration in drinking water for the prevention of dental caries. Public Health Rep. 2015;130(4):318-331. PMID: 26346489 www.ncbi.nlm.nih.gov/pubmed/26346489.
Worthington HV, MacDonald L, Poklepovic Pericic T, et al. Home use of interdental cleaning devices, in addition to toothbrushing, for preventing and controlling periodontal diseases and dental caries. Cochrane Database Syst Rev. 2019;4:CD012018. PMID: 30968949 www.ncbi.nlm.nih.gov/pubmed/30968949.
|
Review Date:
9/2/2019 Reviewed By: Michael Kapner, DDS, General and Aesthetic Dentistry, Norwalk Medical Center, Norwalk, CT. Review provided by VeriMed Healthcare Network. Also reviewed by David Zieve, MD, MHA, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. |
© 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
 All rights reserved.
All rights reserved.