

Asthma in children and adolescents - InDepth
Highlights
The 2020 update to the U.S. National Asthma Education and Prevention Program (NAEPP) guidelines for the diagnosis and management of asthma recommend:
- Patient Education. Patients should be taught skills to self-monitor and manage asthma. Parents should get a written asthma action plan from their children's doctor, which includes information on daily treatment and ways to recognize worsening asthma. Make sure your child's school has a copy of the plan.
- Control of Environmental Factors and Other Asthma Triggers. It is important to reduce exposure to allergens in the home. Treating co-existing chronic conditions (such as rhinitis, sinusitis, and obesity) can help improve asthma control.
- Medications. The NAEPP specifies different treatment plans for children based on three age groups: 0 to 4 years, 5 to 11 years, and 12 years and older. A stepwise approach is recommended where medication types and doses are increased or decreased based on the level of asthma control. The doctor should also monitor the patient's condition to determine when medications should be changed or adjusted.
Symptoms of asthma include:
- Wheezing
- Shortness of breath
- Coughing
- Chest tightness
Exposure before age 1 to pet dander, cockroach, mice allergens, and certain types of household bacteria may actually help protect against the development of wheezing and asthma. Researchers think that exposure to these substances may bolster babies' immune systems. Other research on the "hygiene hypothesis" has suggested that children who grow up on farms also have stronger immune systems due to their exposure to a variety of environmental microorganisms.
Furthermore, prenatal vitamin D supplementation has been found to reduce the chance of asthma and wheezing in the offspring.
Introduction
The word asthma comes from an ancient Greek word meaning panting. Essentially, asthma is an inflammatory lung condition that makes it difficult to breathe properly.
When people inhale, the air travels through the following body structures:
- Air passes through the nose or mouth and then the pharynx (throat) into the lungs through progressively smaller airways called bronchi and then bronchioles. The lungs contain millions of these airways.
- All bronchioles lead to alveoli, which are microscopic sacs where oxygen is taken in and carbon dioxide is expelled.
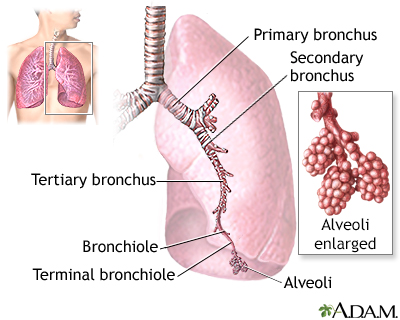
The major features of the lungs include the bronchi, the bronchioles, and the alveoli. The alveoli are the microscopic sacs lined by tiny blood vessels that take in oxygen and give up carbon dioxide.
Asthma is a chronic condition in which these airways undergo changes that are usually triggered by allergens, other environmental triggers, or by infection. Such changes appear to be two specific responses:
- The hyperreactive response (also called hyperresponsiveness)
- The inflammatory response
These actions in the airways cause coughing, wheezing, and shortness of breath (dyspnea), the classic symptoms of asthma.
In the hyperreactive response, smooth muscles in the airways constrict and narrow excessively in response to inhaled allergens or other irritants. This sudden contraction in the muscle walls of the bronchioles is called bronchospasm.
Bronchospasms can result from many different health conditions (allergies, bronchitis, and chronic obstructive pulmonary disease) but asthma is the most common cause.
Everyone's airways constrict when exposed to allergens or irritants, but there are major differences in the hyperreactive response that occurs in people with asthma:
- When people without asthma breathe in and out deeply, their airways relax and open in order to rid the lungs of the irritant.
- When people with asthma try to exhale, their airways do not relax and narrow, causing hyperinflation of the lungs with unexpelled air. As asthma worsens, less air is able to get to the alveoli and the airways narrow further, causing the patients to pant for breath. Smooth muscles in the airways of people with asthma may have a defect, perhaps a deficiency in a critical chemical that prevents the muscles from relaxing. And, during an asthma attack the airways narrow, making breathing difficult.
Hyperreactivity is associated with the inflammatory response, which generally contributes to asthma in the following way:
- The immune system responds to allergens or other environmental triggers by delivering white blood cells and other immune factors to the airways.
- These inflammatory factors cause the airways to swell, fill with fluid, and produce thick, sticky mucus.
- This combination results in wheezing, breathlessness, an inability to exhale properly, and a phlegm-producing cough.
Inflammation appears to be present in the lungs of all patients with asthma, even those with mild cases, and plays a key role in all forms of the disease.

Causes
Doctors do not fully understand the causes of asthma. They believe the disorder is most likely caused by a combination of genetic (inherited) factors and environmental triggers (such as allergens and infections). Asthma tends to run in families. Children whose parents have asthma are more likely to develop it themselves.
Asthma and allergies often coexist, and the allergic response plays a strong role in childhood asthma. About 70% to 85% of children with asthma also have allergies. While only a small percentage of children with allergies have asthma, some of these children may develop asthma as adults.
In people with allergies, the immune system overreacts to exposure to allergens. Allergic asthma is triggered by inhaling certain substances (allergens), such as:
- Dust mites, specifically mite feces, which are coated with enzymes that contain a powerful allergen. These are the primary allergens in the home.
- Animal dander. Cats harbor significant allergens, which can even be carried on clothing; dogs usually cause fewer problems. People with asthma who already have pets and are not allergic to them probably have a lower risk for developing such allergies later on.
- Molds.
- Cockroaches. Cockroach dust is a major trigger and may reduce lung function even in people without a history of asthma.
- Pollen, from nonflowering plants.
An asthma attack can be triggered or aggravated by direct irritants to the lungs. Studies indicate that the more indoor allergens to which a child is allergic, the higher the child's risk for severe asthma. Important irritants include:
- Smoking. Parental smoking can affect the airways in infants as early as their first 2 to 10 weeks of life. Smoking during pregnancy can cause damage in the airways of the developing baby. These babies are at risk for being born with a low birth weight, which affects lung function and increases their risk for asthma.
- Food allergies. Some children with asthma also have food allergies. Research suggests that peanut and milk allergies may increase asthma severity.
- Indoor chemicals. Chemicals used in household cleaning products and furniture materials can trigger asthma.
- Air pollution. Fossil fuels and chemicals that contribute to air pollution may worsen asthma symptoms.
The role of early childhood respiratory and intestinal infections is very complex. Viral respiratory infections certainly worsen existing asthma, but the most common ones are unlikely to cause childhood asthma. In fact, early respiratory and intestinal infections may offer some protection against asthma.
Studies suggest that most respiratory infections are not important causes of asthma in children, except in certain cases. A possible exception is the respiratory syncytial virus (RSV), which is associated with the development of asthma. RSV is the major viral cause of infant pneumonia. Studies also indicate that infants who have reduced lung function within a few days after birth are at increased risk of developing asthma by the time they are 10 years old.
Common respiratory infection viruses that cause colds (such as the rhinovirus) may be associated with the development of asthma in some people. More likely, these viruses do not directly cause asthma, but they worsen asthma in children who already have it. Rhinovirus is the most common infection associated with asthma attacks.
Research indicates that children who have viral-induced wheezing during infancy may be at increased risk for later development of asthma. However, many children outgrow attacks of intermittent wheezing.
The "hygiene hypothesis" theorizes that early exposure to dirt, bacterial germs, and certain infections may help stimulate the immune system to help prevent childhood asthma and allergies. Some studies suggest that children who grow up on farms have lower rates of asthma due to their exposure to a variety of outdoor microorganisms. Other studies indicate that city children exposed before age 1 to cockroaches, mice, and cat dander indoor allergens, and certain types of household bacteria, may also be protected.
It may be that the timing of exposure -- during early infancy -- is a critical factor. Researchers are continuing to explore the hygiene hypothesis and its implications for childhood asthma.
Risk Factors
Asthma affects about 7 million American children. Asthma has dramatically increased over the past few decades in both developed and developing countries around the world. It is now the most common chronic childhood illness.
Most children develop asthma symptoms before they are 5 years old.
Among younger children, asthma is twice as common in boys as in girls, but after puberty it is more common in girls.
Having a parent with asthma increases the risk of developing asthma by 3 to 6 times.
In the US, non-Hispanic Black children have significantly higher rates of asthma than non-Hispanic White children. Both non-Hispanic Black and Hispanic children are more likely to have fatal asthma than non-Hispanic White children. Race and ethnicity are, however, less likely to play a role in these differences in asthma prevalence than socioeconomic factors, such as having less access to optimal health care and a greater likelihood of living in an urban area (another risk factor for asthma). Non-Hispanic White children who live in cities also face a higher risk for asthma.
People with allergic conditions like allergic rhinitis or atopic dermatitis have an increased risk of developing asthma.
Children whose mothers smoked during pregnancy or who were exposed to cigarette smoke secondhand have an increased risk of asthma. Exposure to smog and air pollutants common in the urban environment also increases the risk of developing asthma. [See "Causes" above.]
Certain pregnancy and perinatal factors may possibly be associated with increased risk for asthma, although none are very well studied or proven. Results from studies include:
- Low Birth Weight. Infants of low birth weight are at higher risk for developing lung problems and asthma.
- Winter Birth. Children born in the winter may have a greater risk for asthmatic allergies than children born at other times of the year.
- Breastfeeding. Exclusively breastfeeding for a baby's first 3 months of life may help reduce the risk for wheezing and asthma during early life. However, it is unclear whether the protection will last into later childhood. Breastfeeding has many other benefits for the child. The American Academy of Pediatrics recommends exclusively breastfeeding for a baby's first 6 months of life.
- Complications of Pregnancy. Complications of pregnancy, specifically those involving the mother's uterus (such as post-birth hemorrhage, preterm contractions, insufficient placenta, and restricted growth of the uterus), are associated with an increased risk of childhood asthma.
There is a strong association between obesity and asthma. People who are overweight (body mass index greater than 25) also have more difficulty getting their asthma under control. Weight loss in anyone who is obese and has asthma or shortness of breath helps reduce airway obstruction and improve lung function.
Patients with asthma often also have gastroesophageal reflux disease (GERD), which is associated with acid reflux. It is not entirely clear which condition causes the other or whether they are both due to common factors. Acid reflux can worsen asthma symptoms. Treating GERD may help improve asthma in some patients.
Aspirin-induced asthma (AIA) is a condition in which asthma gets worse after taking aspirin or other nonsteroidal anti-inflammatory drugs (NSAIDs). AIA often develops after a viral infection. It is a particularly severe asthmatic condition, associated with many asthma-related hospitalizations.
Patients with aspirin-induced asthma (AIA) should avoid aspirin and other NSAIDs, including ibuprofen (Advil and other brands, generic) and naproxen (Aleve, generic).
NSAIDs known as COX-2 inhibitors, such as celecoxib (Celebrex), are not associated with aspirin-induced asthma.
In general, children are advised against taking aspirin because of the risk for Reye syndrome, so AIA is uncommon. Acetaminophen appears to be as safe as using ibuprofen and most children with asthma. Tylenol-induced asthma may occur in people with aspirin-induced asthma.
Although this link is not yet proven, parents whose children have asthma should be alert for this possible effect.
Prognosis
Asthma is the third leading cause of hospitalization in children under age 15. The condition can be very serious in children, particularly those younger than age 5, because their airways are very narrow.
Asthma death rates have steadily declined, and asthma is now only rarely fatal in children. Even low mortality numbers are unacceptable, however, since asthma deaths are largely preventable.
Factors associated with an increased risk of death from asthma in children include:
- Previous life-threatening episodes of asthma.
- Two or more hospitalizations or more than three emergency visits in the past year.
- Using two or more short-acting beta2-agonist inhalers per month.
- Lack of adequate and ongoing health care (most likely the reason for the higher fatalities rates in minority children).
- Significant behavioral or psychosocial problems.
- Underestimating the severity of an acute attack -- this poses the greatest threat.
African American children have more than six times the death rate of Caucasians in the age groups of 4 years and younger and 15 to 24 years. Hispanic children also have a higher risk.
Asthma generally improves as children get older, although most school-age children with persistent asthma will still experience symptoms through adolescence. Some children outgrow their asthma by adulthood. In general, the more severe the childhood asthma, the greater the likelihood that it will persist.
Severe asthma can cause long-lasting damage and possibly permanent scarring in some patients. The risk for such injury is highest when asthma strikes children in their first 3 to 5 years. There does not appear to be any significant risk for long-term lung damage for children who develop mild-to-moderate persistent asthma between ages 5 to 12. Children adapt well to living with asthma, and even with severe asthma they can function as well as healthy children in virtually all areas of life.
Symptoms
In children with asthmatic symptoms, it is important to first consider as a possible cause inhaled foreign objects such as peanuts; viral infections such as croup; and bacterial infections, which may be accompanied by high fever and progress rapidly. Any child who has frequent coughing or respiratory infections should be checked for asthma.
The classic symptoms of an asthma attack include:
- Wheezing. Wheezing is nearly always present during an attack. Wheezing is a whistling sound caused by the narrowed airways.
- Shortness of breath (dyspnea). Shortness of breath is a major source of distress in patients with asthma. Breathing may be shallower and more rapid. Use of the muscles at the base of the neck and between the ribs may be more exaggerated than normal. Shortness of breath may worsen during exercise.
- Coughing. In some people, the first (or only) symptom of asthma is a dry cough. Coughing may worsen at night or in the early morning.
- Chest tightness or pain. Initial chest tightness without any other symptoms may be an early indicator of an asthma attack.
Any of these symptoms may worsen with exercise, viral infections, exposure to irritants, stress, or changes in weather.
The end of an attack is often marked by a cough that produces thick, stringy mucus. After an initial acute attack, inflammation lasts for days to weeks, often without symptoms. (The inflammation itself must still be treated, however, because it usually causes relapse.)
The following signs and symptoms may indicate a life-threatening situation:
- Rapid pulse
- Sweating
- Bluish skin color
- Anxiety or panic
- Grogginess, confusion, or difficulty talking
Asthma often progresses very slowly, but it may sometimes develop to a fatal or near-fatal attack within a few minutes. It is very difficult to predict when an attack will become very serious. Any symptoms that suggest a serious attack should be immediately treated with a rescue bronchodilator. If symptoms persist, call for emergency help.
People with a history of a life-threatening asthma attack should carry injectable epinephrine.
Exercise-induced asthma (EIA), also called exercise-induced bronchoconstriction, is a type of asthma in which exercise triggers coughing, wheezing, or shortness of breath. This condition usually occurs during intense exercise in cold dry air. Symptoms start 5 to 10 minutes into exercise and then gradually resolve.
EIA is triggered only by exercise and is distinct from ordinary allergic asthma in that it does not produce a long period of airway hyperactivity, as allergic asthma does. Many people who have allergic asthma also have EIA.

Many patients experience a worsening of their asthma symptoms during the nighttime, especially during sleep. Attacks often occur between 2 and 4 a.m. Factors that increase the risk for nocturnal asthma include allergen exposure, sinus problems, GERD, chronic obstructive lung diseases, and the sleep-disordered breathing associated with obstructive sleep apnea.
Diagnosis
Your child's doctor will want to know any patterns or triggers associated with asthma symptoms. Be sure to let the doctor know:
- Whether symptoms are more frequent during the spring or fall (allergy seasons).
- Whether exercise, a respiratory infection, or exposure to cold air has ever triggered an attack.
- Any family history of asthma or allergic disorders, including eczema, hives, or hay fever.
- Any environmental triggers or other allergic responses.
If symptoms and a patient's history strongly suggest asthma, the doctor will usually perform lung (pulmonary) function tests to confirm the diagnosis and determine the severity of the disease.
A standard test uses a spirometer, an instrument that measures the amount of air taken into and exhaled out from the lungs. The patient breathes into a tube that is connected to a machine. The spirometer can give several measures of airflow:
- Vital capacity (VC), is the maximum volume of air that can be inhaled or exhaled, and is the total lung capacity (TLC). A spirometry test measures the forced vital capacity (FVC), as you breathe into TLC and then do a forced expiration to residual volume.
- Peak expiratory flow rate (PEFR), commonly called the peak flow rate, the maximum flow rate that can be generated during a forced exhalation.
- Forced expiratory volume (FEV1), the maximum volume of air expired (exhaled) in 1 second.
If the airways are obstructed, these measurements will fall. Depending on the results, the doctor will take the following steps:
- If measurements fall, the doctor typically asks the patient to inhale a bronchodilator medication. This drug is used in asthma to open the air passages. The measurements are taken again. If the measurements are more normal, the drug has most likely cleared the airways, and a diagnosis of asthma is strongly suspected.
- If measurement results fail to show airway obstruction, but asthma is still suspected, the doctor may perform a challenge test. It involves administering a specific drug (histamine or methacholine) that usually increases airway resistance only when asthma is present although some other conditions can cause false positive tests.
The doctor may recommend skin or blood allergy tests, particularly if a specific allergen is suspected. Allergy skin tests may help diagnose allergic asthma.
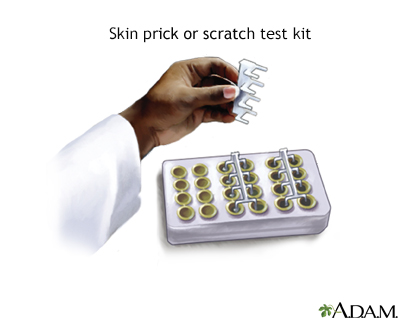
One of the most common methods of allergy testing is the scratch test or skin prick test. The test involves placing a small amount of the suspected allergy-causing substance (allergen) on the skin (usually the forearm, upper arm, or the back), then scratching or pricking the skin so that the allergen is introduced under the skin surface. The skin is observed closely for signs of a reaction, which usually includes swelling and redness of the site. With this test, several suspected allergens can be tested at the same time, and results are usually available within about 20 minutes.
Fractional exhaled nitric oxide (FeNO) tests measure how much nitric oxide is in the air you breathe out. Nitric oxide (NO) is a gas that is considered to be a byproduct of inflammation in the lungs. FeNO can be used when there are doubts about asthma diagnosis in people ages 5 and older.
Other conditions can mimic or worsen asthma and must be ruled out as possible cause of symptoms. They include heart and lung diseases, sinus problems, enlarged thyroid glands, vocal cord dysfunction, infections, and inhaled objects.
Treatment
A stepwise approach is recommended for treating asthma. Medications and dosages are increased when needed, and decreased when possible. Based on a patient's age and asthma severity, there are specific recommendations regarding whether to use long-term control medications and which ones to use. Patient education, environmental control measures, and management of any other conditions are also included.
In choosing therapy, doctors also consider a patient's risk for more severe exacerbations. Contributing factors include parental history of asthma, atopic dermatitis, and known sensitivity to different allergens or foods. Patients should be reevaluated within 2 to 6 weeks of starting therapy to assess response.
While medications play an essential role in the management of asthma, appropriate management of asthma also involves:
- Working with your child's doctor to develop a written Asthma Action Plan that addresses daily maintenance treatment, rescue medications, and what to do if asthma worsens
- Making sure the Asthma Action Plan is on file at your child's daycare, school, and extracurricular activities
- Identifying and avoiding allergens and other asthma triggers, and controlling allergens in the home environment
- Home monitoring, including the use of a peak flow meter
- Communicating regularly with your child's doctor
Doctors classify asthma based on factors such as symptom frequency, nighttime awakenings, lung function, medication need, and normal activity functioning. Asthma severity is generally classified into four groups:
- Intermittent
- Mild Persistent
- Moderate Persistent
- Severe Persistent
Once asthma severity is classified, there is a recommended treatment approach that takes into consideration three age groupings:
- 4 years old or younger
- 5 to 11 years old
- 12 years or older
Key points regarding recommendations for children 4 years old and younger include:
- Long-term control therapy is recommended for children who have had four or more episodes lasting longer than 1 day over the previous year and who have certain risk factors (such as family history of asthma). It may also be considered for other children who are experiencing impairment from their asthma.
- Nebulizers and other devices are available to help administer medications to children this age.
- Only certain inhaled corticosteroids are recommended for these children. Long-acting beta2-agonists are not recommended in children 4 years or younger.
- Close follow-up is recommended.
- Avoidance or management of environmental triggers is always important.
Key points regarding recommendations for children 5 years and older include:
- Participation in physical activities and sports should be encouraged.
- Schools, child care, and camps should all have a copy of the Asthma Action Plan.
- Inhaled corticosteroids are the preferred long-term control therapy. Long-acting beta2 agonists and leukotriene antagonists are additional therapies that may be used in addition to inhaled corticosteroids.
- Avoiding or controlling environmental triggers is always important.
The variation between age groups consists mostly of which medications are recommended and how soon to start various medications and treatments.
Medications for asthma fall into two categories:
- Rescue (Quick-Relief) Medications. Medications that open the airways (bronchodilators or inhalers) are used to quickly relieve any moderate or severe asthma attack. These drugs are usually short-acting beta-adrenergic agonists (beta2-agonists) taken through an inhaler. Beta2-agonists and other rescue medications do not have any effect on the disease process itself. They are useful only for treating symptoms. Frequent need for these medications indicates that the asthma is not well-controlled.
- Long-Term Control (Maintenance) Medications. Long-term control medications focus on controlling the damaging inflammatory response associated with asthma and not simply treating symptoms. For children over age 5 with moderate-to-severe persistent asthma, doctors recommend inhaled corticosteroids, with the addition of long-acting beta2-agonists if necessary.
The goal of asthma therapy is to maximize long-term control of the illness with medications and other treatment approaches, thereby minimizing the frequency of asthma symptoms and asthma attacks. Parents can greatly reduce the frequency and severity of their children's asthma attacks by understanding the difference between coping with asthma attacks and controlling the disease over time.
Unfortunately, many patients do not understand the difference between medications that provide rapid, short-term relief and those that are used for long-term symptom control. It is important not to overuse short-term rescue medications or underuse long-term control corticosteroid medications.
These are the signs of well-controlled asthma:
- Asthma symptoms occur twice a week or less
- Rescue bronchodilator medication is used twice a week or less
- Symptoms do not cause nighttime or early morning awakening
- Symptoms do not limit work, school, or exercise activities
- Peak flow meter readings are normal or the patient's personal best
- Both the doctor and the patient consider the asthma to be well controlled
Most asthma drugs are inhaled. The basic devices used for inhalation are the metered-dose inhaler (MDI), dry powder inhalers, and nebulizers.
Metered-Dose Inhaler
The standard device for administering asthma medication is the metered-dose inhaler (MDI). The medicine comes in a pressurized canister, which is placed inside a plastic inhaler. MDIs, particularly when used with a spacer, allows precise doses to be delivered directly to the lungs.
The spacer is a tube that is attached to the inhaler. It serves as a holding chamber for the medication that is sprayed by the inhaler. The spacer makes it easier and more efficient for the medication to reach the lungs. For children who are too young to breathe into the tube, a face mask can be attached to the spacer.

Dry Powder Inhalers
Dry powder inhalers (DPIs) deliver a powdered form of beta2-agonists or corticosteroids directly into the lungs. Unlike an MDI, dry powder inhalers do not contain a propellant and do not require a spacer. Some patients find that they are more difficult to manage than MDIs. Humidity or extreme temperatures can affect DPIs' performance, so they should not be stored in humid places (bathroom cabinets) or locations subject to high temperatures (glove compartments during summer months).
Dry powder may cause tooth erosion. Children should rinse their mouths out with a fluoride mouthwash right after using these inhalers.
Nebulizers
A nebulizer is a machine that delivers a fine spray of medication-containing liquid. Nebulizers are often used for children younger than 3 years and sometimes for older children who have difficulty using the MDI. It takes 5 to 10 minutes to administer medication using a nebulizer. Because the spray is less targeted than with the inhaler, it must deliver large amounts of the drug. This increases the risk for toxicity and severe side effects. In general, children who can manage an inhaler should not use nebulizers.

Most patients with asthma respond well to standard medications, but a small percentage of people are treatment-resistant. In these cases, a doctor (preferably an asthma specialist) should confirm the asthma diagnosis and evaluate other conditions that might contribute to severe persistent asthma.
Conditions that can worsen asthma include rhinosinusitis, nasal polyps, obesity, obstructive sleep apnea, thyroid dysfunction, and GERD. Medications such as aspirin and other nonsteroidal anti-inflammatory drugs can also worsen asthma. Addressing these conditions can help reduce asthma severity.
For patients age 12 and older who are not helped by high-dose inhaled corticosteroids and long-acting beta agonists, or who require frequent doses of oral steroids, omalizumab (Xolair) may be recommended for patients where allergies play a large role in their asthma.
Patients with increased levels of eosinophils may also benefit from treatment with anti-IL-5 monoclonal antibodies such as mepolizumab (Nucala) or benralizumab (Fasenra), or with anti-IL-4 monoclonal antibodies such as dupilumab (Dupixent).
Quick-Relief (Rescue) Medications
Quick-relief (rescue) medications work immediately to relax airways and quickly control acute asthma attacks. They are not useful for preventing attacks or controlling inflammation in the airways.
The standard quick-relief medication is a beta2-agonist inhaler. Beta2-agonists serve as bronchodilators, relaxing and opening constricted airways during an acute asthma attack. A short-acting inhaled beta2-agonist, taken as needed, is often the only medication used by children with intermittent asthma.
Albuterol (Proventil, Ventolin, Proair), called salbutamol outside the United States, is the standard short-acting beta2-agonist in the United States.
Short-acting bronchodilators are usually administered through inhalation and are effective for 3 to 6 hours. They relieve the symptoms of acute attacks, but they do not control the underlying inflammation. If asthma continues to worsen with the use of these drugs, a doctor may prescribe corticosteroids or other drugs to treat underlying inflammation.
Side Effects of Beta2-Agonists
Side effects of all beta2-agonists may include:
- Anxiety.
- Tremor.
- Restlessness.
- Headache.
- Fast and irregular heartbeats -- notify a doctor immediately if this side effect occurs.
- Children with diabetes or a history of seizures should take these drugs with caution.
- Beta2-agonists have serious interactions with certain drugs; parents should tell the doctor about any other medications their child is taking.
Loss of Effectiveness and Overdose
Short-acting beta2-agonists become less effective when taken regularly over time, which increases the risk for overuse. Overdose can be serious and in rare cases even life threatening.
Common oral corticosteroids include prednisone/prednisolone, dexamethasone, methylprednisolone, and hydrocortisone. They reduce inflammation very effectively. They are most commonly prescribed for asthma flare-ups that do not respond to inhaler medications.
Doctors may provide a written prescription for patients to keep on hand, with specific instructions about when to fill it. Usually, the dosage starts out higher and is gradually reduced over a 5 to 7 day period. Prolonged use of oral steroids has widespread and sometimes serious side effects, so they are not generally given to children for longer than 5 to 7 days.
Asthmanefrin is an over-the-counter (non-prescription) rescue bronchodilator that contains a form of epinephrine called racepinephrine. The medication is inhaled through an atomizer. Asthmanefrin came on the market in 2012 as a replacement for Primatene Mist. (Primatene Mist was discontinued because its inhaler used chlorofluorocarbon (CFC) propellant. CFCs are banned because of environmental concerns.)
Asthmanefrin does not use CFC and is approved for patients ages 4 years and older. However, many doctors have safety concerns regarding the use of epinephrine products for asthma. In particular, this medication can be risky if overused. In general, patients are much better off seeing a health care provider and using inhalers that are prescribed.
Long-Term Control (Maintenance) Medications
Long-term control (maintenance) medications are taken on a regular basis to prevent asthma attacks, control inflammation in the airways, and manage chronic symptoms.
Corticosteroids, also called glucocorticoids or steroids, are powerful anti-inflammatory drugs. Steroids are not bronchodilators (they do not relax the airways) and have little immediate effect on symptoms. Instead, they work over time to reduce inflammation and prevent permanent injury in the lungs. They can also help prevent asthma attacks from occurring.
Taking a corticosteroid drug through an inhaler makes it possible to provide effective local anti-inflammatory activity in the lungs with very few side effects elsewhere in the body. (By contrast, oral steroids have considerable side effects throughout the body.) Inhaled corticosteroids (ICS) are recommended as the primary therapy for any patient needing long-term control medications for persistent asthma.
Examples of inhaled corticosteroids:
- Beclomethasone (QVAR), budesonide (Pulmicort), ciclesonide (Alvesco), flunisolide (AeroBid), fluticasone (Flovent), mometasone furoate (Asmanex), and triamcinolone (Azmacort and others).
- Budesonide (Pulmicort Respules) is available in a jet nebulizer for children ages 12 months to 8 years. It was the first such medication to be approved for children in this age group.
- Inhalers that combine both long-acting beta2-agonists and corticosteroids are also available. These include Symbicort (budesonide/formoterol), fluticasone-salmeterol (Advair), and mometasone-formoterol (Dulera).
Inhaled corticosteroids are the preferred first-line therapy for children with asthma. However, doctors caution against corticosteroids for infants and toddlers with mild asthma and urge close monitoring, especially for children under age 5 with severe asthma who are receiving high doses.
Inhaled corticosteroids and growth in children is a common concern. However, a number of studies report only a slight effect (about half an inch or 1.25 centimeters) on children's growth, which may be only temporary. These growth changes are mostly when higher doses are being used. Poorly controlled asthma can also affect growth.
Side effects of inhaled steroids may include:
- Throat irritation, hoarseness, and dry mouth (the most common side effects). Using a spacer device and rinsing the mouth after each treatment can minimize or prevent these effects.
- Rashes, wheezing, facial swelling (edema), fungal infections (thrush) in the mouth and throat, and bruising are also possible, but not common, with inhalers.
- Some studies have suggested a higher risk for gum inflammation.
- It is not yet known whether inhaled steroids affect lung development in very young children. Steroids administered using nebulizers are of particular concern.
There are two types of long-acting bronchodilators:
- Long-acting beta2-agonists (LABAs)
- Long-acting muscarinic antagonists (LAMAs)
Long-acting beta2-agonists (LABAs) are used for preventing an asthma attack (not for treating attack symptoms). These drugs should never be used alone in the treatment of asthma in adults or children. They can be dangerous when used alone, because they can mask asthma symptoms, and they can increase the risk of asthma death unless paired with an inhaled steroid. LABAs should only be used in combination with an asthma controller medication, such as an inhaled corticosteroid. LABAs should be used for the shortest time possible, and should only be used by patients whose asthma is not adequately controlled by asthma controller medications.
Salmeterol-fluticasone (Advair), formoterol-budesonide (Symbicort), and mometasone-formoterol (Dulera) are long-acting beta2 agonists products combined with a steroid in a single inhaler that are used for treatment of moderate-to-severe asthma. Advair is approved for children ages 4 years and older, and Symbicort and Dulera are approved for children ages 12 years and older.
Long-acting muscarinic antagonists (LAMAs) are other long-acting bronchodilator drugs. Like LABAs, LAMAs are used to prevent asthma attacks rather than to treat attack symptoms. Also like LABAs, LAMAs are not used by themselves, but in combination with corticosteroids. Although LABAs are preferred over LAMAs when corticosteroids alone do not control asthma, if a LABA cannot be used or is not available, LAMAs can be used instead. LAMAs can also be used in addition to corticosteroids and LABAs when this combination is not sufficient to control asthma symptoms.
Examples of LAMAs include umeclidinium (Incruse), glycopyrrolate (Seebri), tiotropium (Spiriva) and aclidinium (Tudorza).
Combination LAMA/LABA inhalers include umeclidinium/vilanterol (Anoro) and tiotropium/olodaterol (Stiolto).
Leukotriene antagonists (also called anti-leukotrienes or leukotriene modifiers) are oral medications used for prevention, NOT for treating acute asthma attacks.
Leukotriene antagonists include montelukast (Singulair, generic) and zafirlukast (Accolate, generic). Zileuton (Zyflo) is a leukotriene inhibitor. These drugs are considered an alternative for long-term control of asthma. Other potential uses include preventing exercise-induced asthma.
Side Effects and Complications
Upset stomach, headache, and sore throat are the most common side effects of leukotriene antagonists. Because zafirlukast and zileuton can raise liver enzyme levels, patients on these medicines may need periodic liver tests.
Leukotriene antagonists may cause mental health and behavioral changes. Mood problems include agitation, aggression, anxiousness, dream abnormalities, hallucinations, depression, insomnia, irritability, restlessness, tremor, and suicidal thinking. Patients who take a leukotriene antagonist drug should be monitored for signs of behavioral and mood changes. Doctors should consider discontinuing the drug if patients exhibit any of these symptoms.
Omalizumab (Xolair) is FDA-approved for patients age 12 and older. It should be considered only for children over 12 years who have moderate-to-severe persistent asthma related to allergies and for adults who have severe asthma and allergies. Omalizumab is a biologic drug that targets and blocks the antibody immunoglobulin E (IgE), a chemical trigger of the inflammatory events associated with an allergic asthma attack.
Omalizumab is given by injection every 2 to 4 weeks. It is used only to treat patients whose symptoms are not controlled by inhaled corticosteroids.
Side Effects and Complications
About 1 in 1,000 patients who take omalizumab develop anaphylaxis (a life-threatening allergic reaction). Patients can develop anaphylaxis after any dose of omalizumab, even if they had no reaction to a first dose. Anaphylaxis may occur up to 24 hours after the dose is given.
Omalizumab should always be injected in a doctor's office and health care providers should observe patients for at least 2 hours after an injection. Patients should also carry emergency self-treatment for anaphylaxis (such as an Epi-Pen) and know how to use it. With an Epi-Pen, or similar auto-injector device, patients can quickly give themselves a life-saving dose of epinephrine.
Anaphylaxis symptoms include:
- Difficulty breathing
- Chest tightness
- Dizziness
- Fainting
- Itching and hives
- Swelling of the mouth and throat
The FDA is currently reviewing whether omalizumab may be associated with increased risk for heart and vascular problems (ischemic heart disease, arrhythmias, cardiomyopathy, heart failure, pulmonary hypertension, and blood clots).
Mepolizumab (Nucala) and benralizumab (Fasenra) are anti-IL-5 monoclonal antibodies FDA-approved for patients 12 years and older with severe asthma and with an eosinophilic phenotype. Generally, patients who have a high level of eosinophils are predicted to have a good response to anti-IL-5 therapy. These drugs decrease eosinophil differentiation, maturation, and migration and have demonstrated efficacy in reducing exacerbations in patients with severe asthma. They are a form of maintenance therapy and are not meant to be used in acute exacerbations or in patients with status asthmaticus.
Mepolizumab and benralizumab are administered once every 4 weeks via subcutaneous injection. Severe allergic reactions are possible, so injections are usually given in a provider's office and patients monitored for allergic reactions. Some patients treated with mepolizumab (Nucala) have experienced opportunistic infections such as shingles or herpes zoster.
Theophylline relaxes the muscles around the bronchioles and also stimulates breathing. Since the introduction of inhaled corticosteroids and long-acting beta2-agonists, theophylline is not used as often for asthma treatment. It may still be used in some circumstances, such as for treating severe or nocturnal asthma. Theophylline is available in tablet, liquid, and injectable forms. Theophylline should not be used by people with peptic ulcers or GERD, and should be used with caution by anyone with heart disease, liver disease, high blood pressure, or seizure disorders.
If a child is taking theophylline on an ongoing basis, the doctor should monitor the drug level at the start of therapy and at regular intervals thereafter.
Other Treatments
Children older than 6 months should receive an influenza vaccination every year. All children should receive pneumococcal vaccination. The pneumococcal conjugate vaccination (PCV13) is recommended for children younger than 5 years old. Children age 2 years and older who are at high risk for pneumococcal disease should also get the pneumococcal polysaccharide vaccine (PPSV23).
Treatment of allergies and sinusitis can help control asthma.
Patients with asthma and chronic allergic rhinitis may need daily medications. Patients with severe seasonal allergies may need to start taking medications a few weeks before the pollen season, and to continue them until the season is over.
Immunotherapy ("allergy shots") may help reduce asthma symptoms, and the use of asthma medications, in patients with known allergies. They may also help prevent the development of asthma in children with allergies. Immunotherapy poses some risk for severe allergic reactions, especially for children with poorly controlled asthma, so it is important that the doctor carefully evaluates the child's asthma condition.
The latest guidelines indicate that immunotherapy injections for treatment of allergies are safe for young children.
Researchers are studying an oral form of immunotherapy that uses a sublingual (under-the-tongue) tablet. Some, but not all, sublingual tablets are approved for children older than 10 years. Recent studies indicate that sublingual therapy may be helpful for asthma. However, questions still remain including dosage and duration of treatment. Sublingual therapy has recently been FDA-approved for allergic rhinitis. At this time, sublingual immunotherapy is not approved or recommended for asthma treatment in the United States.
Respiratory infections, including the common cold, can interact with allergies to worsen asthma. People with asthma should try to minimize their risk for respiratory tract infections. Using alcohol-based hand rubs and washing hands are simple but effective preventive measures. Vaccines are also very important for prevention.
Children with obvious symptoms of reflux (heartburn) or children who have difficulty managing asthma may consider the following lifestyle changes:
- Avoiding heavy meals and meals with fried food.
- Avoiding caffeine products (cola drinks and chocolate), garlic, and onions.
- Avoiding eating or drinking at least 3 hours before bedtime.
- Elevating the head of the bed by 6 inches.
- Medications are available for treating gastroesophageal reflux but should be discussed with your child's doctor. The use of PPI drugs to improve asthma symptoms is controversial. Studies indicate that these drugs do not help with asthma symptoms.
Many people with asthma turn to alternative therapies including high-dose vitamins, homeopathic remedies, probiotics, and herbal supplements. There is no evidence that any of these treatments are helpful for asthma.
However, because stress can worsen asthma symptoms and make breathing more difficult, alternative therapies that focus on relaxation and stress reduction may be helpful. These modalities include:
- Breathing and relaxation techniques, including meditation and yoga
- Biofeedback
- Hypnosis
- Acupuncture
- Massage therapy
Managing Asthma At Home
The more allergies a child has, the more severe the asthma. Making lifestyle changes to reduce allergy attacks and other triggers is extremely important.
Asthma action plans create a written document for patients and parents to manage asthma during stable times and to more easily identify when asthma is worsening. Important components of a home program include:
- A clearly written plan for taking asthma medications when condition is stable.
- Instructions for what medicines to take if asthma gets worse.
- Education regarding the difference between long-term control medications and quick-relief medications.
- Monitoring of asthma on a daily basis. Symptom monitoring is adequate for patients with intermittent or mild persistent asthma. Peak flow monitoring should be performed in patients with moderate or severe persistent asthma or those with a history of more severe exacerbations (sudden worsening or increase in severity of symptoms).
- A list of environmental control measures that need to be taken to control exposure to allergens.
- When to seek medical care.
A peak flow meter is a handheld plastic device for measuring peak expiratory flow rate (PEFR). PEFR measures how fast you can expel air out of your lungs and is an indication of lung functioning. Changes in the PEFR may indicate problems with asthma control even before symptoms appear. If your child's PEFR is lower than normal, it may mean that rescue medications are needed.
It is a good idea to keep a written record of your child's peak flow meter readings. This data can help the doctor adjust medications and recognize problems before they become serious.
To use a peak flow meter, set the meter to zero and have your child stand or sit upright, take a deep breath and exhale hard and fast into the meter. Write down the number that appears on the meter.
House dust is a reservoir for pollen and dust mites. It is important to control household allergens and pollutants in the home.
Controlling for Dust
Spray furniture polish is very effective for reducing both dust and allergens. Air purifiers and vacuum cleaners with High Efficiency Particular Air (HEPA) filters can help remove particles and small allergens found indoors. Neither vacuuming nor the use of anti-mite carpet shampoo, however, is effective in removing mites in house dust. In fact, vacuuming stirs up both mites and cat allergens. If possible, avoid carpets and rugs.

Controlling Pets
For children who have an existing allergy to pets:
- If possible, keep pets outside.
- If this is not possible, confine pets to carpet-free areas outside the bedroom. Cats harbor significant allergens, which can even be carried on clothing. Dogs usually cause fewer problems.
- Wash animals once a week to reduce allergens. Dry shampoos, available for both cats and dogs, can remove allergens from the skin and fur and are easier to administer than wet shampoos.
Bedding, Curtains, and Bedroom Environment
- Replace curtains with shades or blinds, and wash bedding using the highest temperature setting.
- Encase mattress and pillow in special dust mite proof covers (synthetic pillows may pose a higher risk for asthma attacks than feather pillows, or no pillow at all).
- Wash pillows in water hotter than 130°F (55°C), or in cooler water with detergent and bleach.
- Wash sheets and blankets weekly in hot water.
- Avoid sleeping or lying on cushions or furniture that are cloth covered.
- Keep stuffed toys away from the bed and wash them weekly in hot water. Placing toys in a dryer or freezer may help, but is not as helpful as washing.
- Avoid the bottom bunk of the bunk bed. In general, children should sleep as high off the floor as possible.

Exterminating Pests (Cockroaches and Mice)
- Use professional exterminators to eliminate cockroaches. Cleaning the house using standard housecleaning techniques may not eliminate the cockroach allergens themselves.)
- Exterminate mice, and attempt to remove all dust, which might contain mouse urine and dander.
- Keep food and garbage in closed containers.
- Keep food out of bedrooms.
Reducing Humidity in the House
Living in a damp environment is counterproductive. Humidity levels should not exceed 30% to 50%.
- Fix all leaky faucets and pipes, and eliminate collections of water around the outside of the house.
- Dehumidify basements, but empty dehumidifiers and clean them daily with vinegar solution.
- Clean often any moldy surfaces in the basement or in other areas of the home.
- Avoid prolonged use of vaporizers to manage symptoms during asthma attacks.
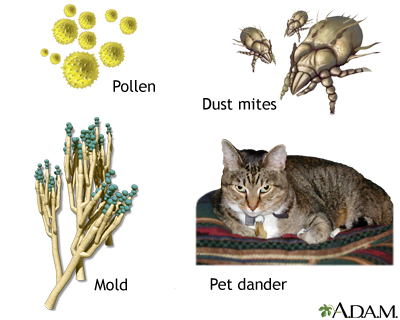
Many of the same substances trigger both allergies and asthma. Common allergens include pollen, dust mites, mold, and pet dander. Other asthma triggers include irritants like smoke, pollution, fumes, cleaning chemicals, and sprays. Avoiding exposure to known allergens and respiratory irritants can substantially reduce asthma symptoms.
Preventing Exposure to Cigarette and Cooking Smoke
Parents who smoke are strongly urged to quit. Studies indicate that exposure to second-hand smoke in the home increases the risk for asthma and asthma-related emergency room visits in children. Even smoky cooking can worsen asthma.
Avoiding Outdoor Allergens
The following are some recommendations for avoiding allergens outside:
- Avoid scheduling camping and hiking trips during times of high pollen count (generally, May and June for grass pollen and mid-August to October for ragweed in the eastern half of the United States).
- Avoid strenuous activity when ozone levels are highest, which usually occur in early afternoon, particularly on hot hazy summer days. Levels are lowest in early morning and at dusk.
- Asthma attacks are often triggered by thunderstorms. It is not clear why. Some evidence points to a build-up of ozone that accompanies such storms. Mold exposure can play a role.
- Patients who are allergic to mold should avoid barns, hay, raking leaves, and mowing grass. Exposure to automobile fumes may worsen asthma. Fungi in car air conditioners can also be a problem.
- Air pollution can worsen existing asthma. Avoid strenuous activity during times of high air pollution.
Parents should make sure that their child's school has a copy of the written asthma action plan. The plan should contain a list of medications the child takes (including which ones need to be taken during school hours), identified asthma triggers, and emergency contact numbers. Parents should also make sure that the school staff is trained in the steps to take in case of an asthma attack.
Asthma is no reason to avoid exercise. Historically, about 10% of Olympic athletes have asthma. Some studies indicate that long-term exercise may help control asthma and reduce hospitalization. Exercise can help control weight, which can help with asthma symptoms.
Encourage children with asthma to swim and play sports, such as baseball, that will be less difficult for them. Intense activities lasting less than 2 minutes, such as sprinting or competitive swimming, may cause fewer problems than longer-lasting exercises.
Young people who enjoy running should probably choose an indoor track to avoid pollutants. Swimming is excellent for people with asthma. Yoga, which uses stretching, breathing, and meditation techniques, may also have particular benefits.
Patients should consult their doctors before starting any exercise program. Exercise-induced asthma (EIA) is a limited condition that has specific recommendations.
Hints for Reducing Exercise-Induced Asthma (EIA)
EIA occurs within the first 5 to 10 minutes of exercise and is more likely to occur with regular paced activities in cold, dry air. The following are some suggestions for reducing its impact:
- Warm-up and cool-down before and after exercise.
- Choose activities that do not require exposure to cold, dry air.
- Participate in activities with short bursts of exercise (such as tennis and football) rather than exercises involving long-duration pacing (such as cycling, soccer, and distance running).
- Breathe through a scarf or through the nose. This helps warm up the airways when exercising in cold air.
- Use any prescribed medications as directed.
Medications for EIA
Treatment guidelines for exercise-induced asthma recommend:
- A short-acting beta2-agonist (albuterol) taken 15 minutes before exercise is the first choice, and lasts for 2 to 3 hours.
- A leukotriene antagonist drug taken daily is the second choice for patients who continue to have exercise asthma symptoms. These patients should also use daily an inhaled steroid for maintenance control.
Asthma can trigger a difficult emotional-physical cycle:
- Breathlessness and wheezing produce a fear of suffocation and death, even in very small children.
- This anxiety makes the muscles surrounding the airways even tighter, which makes breathing even more difficult.
Caregivers must first focus on reducing their own anxiety, which can heighten a child's own fears. The next step is to help the child relax. One method for this is as follows:
- The child sits comfortably, bending slight forward with the eyes closed and hands placed gently above the navel.
- Tell the child to pretend the stomach is a balloon.
- The "balloon" must be "blown up" by inhalation, not exhalation. The child can tell if this working because the hands will move slightly apart.
- When the child breathes out, the "balloon" will be made flat.
This exercise both relaxes the child and discourages shallow, oxygen-poor breathing. Massaging the child in gentle circles on the chest is relaxing and may also loosen mucus.
Other recommendations to provide relief include:
- Place the child stomach-down on several pillows so that the head is slightly lower than the chest. Gently pat the child's back between the shoulder blades.
- Warm liquids, such as soup or hot cider, can help loosen mucus and may also relax bronchial muscles. Cold fluids, like cold air, should be avoided.
- Overhydration (too much liquid) can be harmful, however, so these drinks should not be forced on the child.
- Warm, moist air from vaporizers can greatly ease and moderate asthma attacks.
Home visits by a nurse or other health care provider may be helpful if your family is having trouble managing your child's asthma or following prescribed treatments. It is also a good idea to have your home evaluated for allergic triggers.
Resources
- The American Lung Association -- www.lung.org
- American College of Allergy, Asthma & Immunology -- acaai.org
- American Academy of Allergy, Asthma, and Immunology -- www.aaaai.org
- National Heart, Lung, and Blood Institute -- www.nhlbi.nih.gov
- Asthma and Allergy Foundation of America -- www.aafa.org
References
Bardin PG, Price D, Chanez P, Humbert M, Bourdin A. Managing asthma in the era of biological therapies. Lancet Respir Med. 2017;5(5):376-378. PMID: 28463176 pubmed.ncbi.nlm.nih.gov/28463176/.
Boulet LP, O'Byrne PM. Asthma and exercise-induced bronchoconstriction in athletes. N Engl J Med. 2015;372(7):641-648. PMID: 25671256 pubmed.ncbi.nlm.nih.gov/25671256/.
Brozek JL, Bousquet J, Agache I, et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines-2016 revision. J Allergy Clin Immunol. 2017;140(4):950-958. PMID: 28602936 pubmed.ncbi.nlm.nih.gov/28602936/.
Bush A, Fleming L, Saglani S. Severe asthma in children. Respirology. 2017;22(5):886-897. PMID: 28543931 pubmed.ncbi.nlm.nih.gov/28543931/.
Cloutier MM, Dixon AE, Krishnan JA, Lemanske RF Jr, Pace W, Schatz M. Managing asthma in adolescents and adults: 2020 asthma guideline update from the National Asthma Education and Prevention Program. JAMA. 2020;324(22):2301-2317. PMID: 33270095 pubmed.ncbi.nlm.nih.gov/33270095/.
Del Giacco SR, Bakirtas A, Bel E, et al. Allergy in severe asthma. Allergy. 2017;72(2):207-220. PMID: 27775836 pubmed.ncbi.nlm.nih.gov/27775836/.
Durani SR, Bacharier LB, Guilbert TW. Diagnosis of asthma in infants and children. In: Burks AW, Holgate ST, O'Hehir RE, et al, eds. Middleton’s Allergy: Principles and Practice. 9th ed. Philadelphia, PA: Elsevier; 2020:chap 49.
Expert Panel Working Group of the National Heart, Lung, and Blood Institute (NHLBI) administered and coordinated National Asthma Education and Prevention Program Coordinating Committee (NAEPPCC), Cloutier MM, Baptist AP, Blake KV, et al. 2020 focused updates to the asthma management guidelines: a report from the National Asthma Education and Prevention Program Coordinating Committee Expert Panel Working Group. J Allergy Clin Immunol. 2020;146(6):1217-1270. PMID: 33280709 pubmed.ncbi.nlm.nih.gov/33280709/.
Farne HA, Wilson A, Powell C, Bax L, Milan SJ. Anti-IL5 therapies for asthma. Cochrane Database Syst Rev. 2017;9:CD010834. PMID: 28933516 pubmed.ncbi.nlm.nih.gov/28933516/.
Fuchs O, Bahmer T, Rabe KF, von Mutius E. Asthma transition from childhood into adulthood. Lancet Respir Med. 2017;5(3):224-234. PMID: 27666650 pubmed.ncbi.nlm.nih.gov/27666650/.
Jackson DJ, Lemanske RF, Bacharier LB. Management of asthma in infants and children. In: Burks AW, Holgate ST, O'Hehir RE, et al, eds. Middleton's Allergy: Principles and Practice. 9th ed. Philadelphia, PA: Elsevier; 2020:chap 50.
Maloney J, Prenner BM, Bernstein DI, et al. Safety of house dust mite sublingual immunotherapy standardized quality tablet in children allergic to house dust mites. Ann Allergy Asthma Immunol. 2016;116(1):59-65. PMID: 26553448 pubmed.ncbi.nlm.nih.gov/26553448/.
Mauer Y, Taliercio RM. Managing adult asthma: The 2019 GINA guidelines. Cleve Clin J Med. 2020;87(9):569-575. PMID: 32868307 pubmed.ncbi.nlm.nih.gov/32868307/.
Ramratnam SK, Bacharier LB, Guilbert TW. Severe asthma in children. J Allergy Clin Immunol Pract. 2017;5(4):889-898. PMID: 28689839 pubmed.ncbi.nlm.nih.gov/28689839/.
Sobieraj DM, Baker WL, Nguyen E, et al. Association of inhaled corticosteroids and long-acting muscarinic antagonists with asthma control in patients with uncontrolled, persistent asthma: A systematic review and meta-analysis. JAMA. 2018;319(14):1473-1484. PMID: 29554174 pubmed.ncbi.nlm.nih.gov/29554174/.
Sobieraj DM, Weeda ER, Nguyen E, et al. Association of inhaled corticosteroids and long-acting ß-agonists as controller and quick relief therapy with exacerbations and symptom control in persistent asthma: A systematic review and meta-analysis. JAMA. 2018;319(14):1485-1496. PMID: 29554195 pubmed.ncbi.nlm.nih.gov/29554195/.
van de Griendt EJ, Tuut MK, de Groot H, Brand PLP. Applicability of evidence from previous systematic reviews on immunotherapy in current practice of childhood asthma treatment: a GRADE (Grading of Recommendations Assessment, Development and Evaluation) systematic review. BMJ Open. 2017;7(12):e016326. PMID: 29288175 pubmed.ncbi.nlm.nih.gov/29288175/.
von Mutius E, Smits HH. Primary prevention of asthma: from risk and protective factors to targeted strategies for prevention. Lancet. 2020;396(10254):854-866. PMID: 32910907 pubmed.ncbi.nlm.nih.gov/32910907/.
Woodruff PG, Bhakta NR, Fahny JV. Asthma: pathogenesis and phenotypes. In: Broaddus VC, Mason RJ, Ernst JD, et al, eds. Murray and Nadel's Textbook of Respiratory Medicine. 6th ed. Philadelphia, PA: Elsevier Saunders; 2016:chap 41.
Reviewed By: Stuart I. Henochowicz, MD, FACP, Clinical Professor of Medicine, Division of Allergy, Immunology, and Rheumatology, Georgetown University Medical School, Washington, DC. Also reviewed by David Zieve, MD, MHA, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.